A new study published in the current New England Journal of Medicine assessed the outcomes of total knee replacement surgery (along with standard modalities, including pain medications and physical therapy when indicated) against intensive physical therapy alone. The study included 50 surgical patients as compared with 50 treated solely with "conservative" (non-surgical) methods: weight loss, supervised exercise and physical therapy, along with medication as needed.
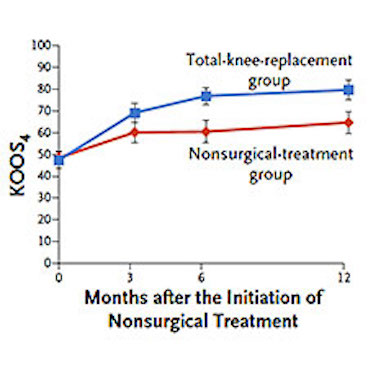
In patients with knee osteoarthritis, total knee replacement followed by nonsurgical treatment resulted in greater pain relief and functional improvement after 12 months than did nonsurgical treatment alone. However, surgery was associated with a higher number of serious adverse events.
The authors, led by Saran T. Skou of the Institute of Sports Science and Clinical Biomechanics, University of Southern Denmark, Odense, found that 85 percent of the total knee replacement (TKR) group had significant (>15 percent) pain relief and functional improvement. However, the same was true for 68 percent of those who did not have surgery. It is a notable difference, but digging deeper in the data the picture becomes murky.
First, the surgical group had 8 serious complications (that's 16 percent of 50 patients, not insubstantial): 3 experienced DVTs (vein clots, potentially lethal), 1 each of deep tissue infection and bony fracture, and 3 experienced severe stiffness requiring manipulation under anesthesia. Meanwhile, the non-operated group had none of those.
On the other hand, 13 control patients (26 percent) elected to undergo TKR before the one-year mark, and it's quite possible that more will decide to in the near future. And of course it's unknown how long the benefits of non-surgical treatments will endure.
As noted by Dr. Jeffrey Katz in his accompanying editorial:
Nearly 1 million elective total knee and hip replacements are performed annually in the United States; rates of total knee replacement tripled in the past 20 years and are projected to increase further. More than 90% of total knee replacements are performed for knee osteoarthritis, which affects approximately 14% of adults in the United States in their lifetimes. Prior to the introduction of total knee replacement in the 1970s, patients with advanced knee osteoarthritis frequently became housebound; now such patients can remain mobile.
This study was too small by far to really end the need for more, larger studies, and there's no way these 100 patients can be used to do the needed sub-group analyses. The placebo effect may also confound both arms of this study. The dramatic improvements in pain and mobility from TKR will likely continue to persuade most arthritic patients to undergo the procedure, and nothing in this study should dissuade them. Others who are more risk-averse may elect the non-surgical approach, knowing that they can choose surgery later on. As always, what's needed is an informed discussion between doctor and patient.


