We left off about to explore recommendations “that either improve the supply of new antimicrobial medicines or reduce the demand for existing ones, prolonging their life.”
“AMR is inevitable. As people keep finding ways to kill the microbes that infect us, those microbes, through evolutionary processes, will mutate to counteract them. …we can reduce the build-up of resistance by reducing unnecessary use of antimicrobials and in particular antibiotics. This is important because the supply of new antimicrobials is not necessarily inexhaustible, whilst their development is increasingly expensive.”
Addressing the issues of the demand side are a bit easier to understand and the recommendations more direct. There are three sources of antimicrobial waste entering the environment interacting with microbes; from our use in animals and humans and manufacturing antimicrobials. The majority of antimicrobials given to animals and humans is excreted unmetabolized to enter our waste systems, with smaller amounts contributed by outdated or unused antimicrobials dumped by patients and healthcare systems.
Active pharmaceutical ingredients or APIs are biologically active components of drugs. As the New York Times has reported “The critical ingredients for most antibiotics are now made almost exclusively in China and India. While APIs are manufactured to global standards, the UK review indicates “there is growing evidence that some API manufacturers do not adequately treat waste products, with the result that antibiotic APIs are released into the local environment, usually as waste water.”
An economically driven recommendation is that the end manufacturer, the pharmaceutical companies selling the drugs be held accountable for driving higher standards “through their supply chains” – in the way we have asked Apple to improve employment standards by their Chinese suppliers.
These sources of waste can dramatically decrease if a greater driver of demand, the inappropriate use of antimicrobials was better controlled. While acknowledging the need for antibiotics “to maintain animal welfare and food security,” the report condemns the use of antibiotics as prophylaxis or to promote growth. The report points out that the FDA’s finding that 70% (by weight) of antibiotics defined as medically important for humans are used in animals.
Physicians overprescribe antimicrobials because of errors in diagnosis e.g. treating a viral infection with an antibacterial agent, demands by patient’s for treatment, and government mandate. Even though the United States agrees on a global level for the need to control AMR; CMS requires hospitals to begin antibiotic therapy for pneumonia within an hour of the patient’s arrival in the emergency department. There is no test currently available reliably guiding treatment – acceptable antibiotic choice is dictated nationally. In how many instances is this policy, with all its good intents for patient care, driving AMR by mistakenly treating viral pneumonia or congestive heart failure with antibiotics? The absence of inexpensive, rapid, reliable clinical tests to guide microbial use are an underlying cause of over-prescription. Jim O’Neil writes
“I find it incredible that doctors must still prescribe antibiotics based only on their immediate assessment of a patient’s symptoms, just like they used to when antibiotics first entered common use in the 1950s. When a test is used to confirm the diagnosis it is often based on a slow technology that hasn’t changed significantly since the 1860s. I can understand why this is the situation: there aren’t enough good and rapid tests to confirm the professional judgment of the doctor, and the tests that are available are often more expensive than prescribing the drugs ‘just in case’. Yet this is not acceptable.”
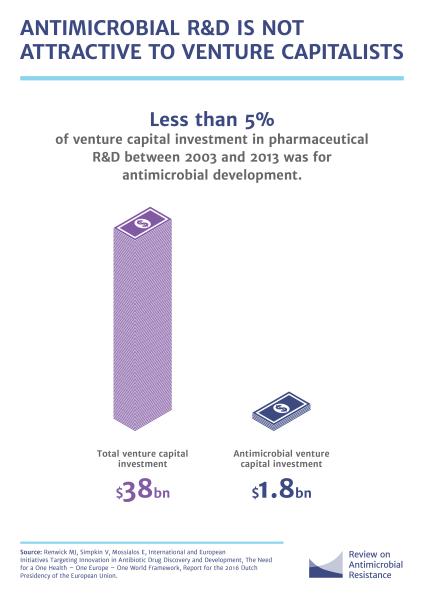
On the supply side of the equation, there is a mismatch between the drugs we need and those researched. Currently, there are about 40 products under development many targeted at easier-to-treat, more lucrative infections. There are scientific challenges to be sure, but the economic bias of the report returns consideration to market conditions and the regulatory environment.
The entry of a new antimicrobial into the marketplace has its specific features. There is uncertainty as to how antimicrobial resistance will develop, what needs it will create; and this coupled with our current regulatory system creates a 10-15 year cycle from discovery to market. The regulatory environment is justifiably robust; we want effective, not deleterious drugs. But it 's hard logistically to conduct trials of ‘clinical superiority’ for drug-resistant therapies. These factors make it difficult to quickly adapting to antimicrobial resistance. And it may be difficult to recoup R&D costs for a new antimicrobial; first, because sales volumes are less than established branded and generic drugs and second because responsible stewardship limits the use of “newer drugs, so as to slow the emergence of resistance to them and prolong their usefulness.”
The UK recommendation at the heart of delinking drug development costs from the sale price, removes volume considerations, reduces “uncertainty and enabling reward without encouraging poor stewardship.” They propose ‘market entry awards’ of $800 million to $1.3 billion for antimicrobials designed to address defined current and future need. The reward or incentive would be linked to the product’s value to society and with a “quid pro quo for receiving a lump sum payment should be a broad commitment to continued development post-approval and responsible sale and marketing of the product. … ensuring global, affordable access to the product.”
The UK’s report, A review of Antimicrobial Resistance, is a well-considered blueprint of a financially viable way forward. While it may not find its way to your nightstand, it should be required reading for our legislatures. On a hopeful note, the Financial Times reports that 13 members of Big Pharma have already signed on.
.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


