A new paper in JAMA Cardiology titled Long-term Safety and Efficacy of Achieving Very Low Levels of Low-Density Lipoprotein Cholesterol found that very aggressive lowering of LDL-C (bad cholesterol) was not associated with an increased incidence of safety problems and demonstrated that the efficacy composite of cardiovascular death, major coronary events, and stroke were ‘significantly’ lower.
This has been a concern from some.
Here is the science:
- It was a data mining expedition into the Improve-it Trial – the Vytorin Efficacy International Trial, which looked at the effect of LDL-C-reducing therapy with ezetimibe/simvastatin compared with simvastatin alone in 18,144 patients who had had an acute coronary event.(ACS) Acute coronary syndrome (ACS) is the actual term and refers to a spectrum of clinical presentations ranging from myocardial infarction to unstable angina.
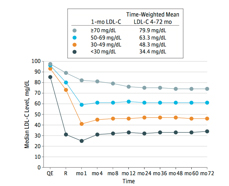
- The patients were stratified based upon their achieved LDL-C after one month of intervention. They are listed in the accompanying graphic.
- Those who achieved an LDL-C of 30mg/dL were more likely male, nonwhite, had higher body mass index, and more liable to have preexisting diabetes, less likely to be a smoker or to have had a prior myocardial infarction, percutaneous coronary intervention, or coronary artery bypass surgery. Additionally, they were also the least likely to have been treated with A statin before their qualifying ACS event, and they had the lowest median LDL-C level at baseline of the four groups.
- 9.5% of patients had an adverse event leading to drug discontinuation — essentially the same in each group
- There was no difference in the percentage of patients experiencing muscular difficulties (myopathy, myalgia or rhabdomyolysis), liver dysfunction, biliary disease, neurocognitive events (short or long term), hemorrhagic stroke, hospitalization for heart failure, noncardiac deaths or cancer for any of the four LDL-C groupings.
- In conclusion, we observed that the achievement of very low LDL-C concentration at 1 month in a cohort of 971 patients followed up for a median of 6 years experienced a generally similar safety profile as those with higher LDL-C levels, and that achievement of LDL-C levels below currently recommended targets was associated with even further numerical reductions in cardiovascular events. These observational data support the use of intensive lipid lowering in very high-risk patients following an ACS to prevent future ischemic events.
So the bottom line is that cardiologists are willing to move the LDL-C goalposts once again. The previous aggressive value of 70mg/dL is giving way to a new lower value because it has an acceptable safety profile and further reductions in cardiovascular events. The recent announcement of the results of a new cholesterol medication, Repatha demonstrated LDL-C levels much lower than the currently clinically accepted values of 70mg/dL.
But the further reductions come at a cost, that is what I recently reported in reviewing the Repatha study.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


