
Let's give a (non) round of applause to the CDC. I have written many times about how the agency's bungling of the opioid overdose epidemic by "solving" the wrong problem has only succeeded in making things worse. (See: How the feds are fueling America’s opioid disaster.)
Data from all over the US makes it patently obvious that opioid pills are not the driver of overdose deaths, which have skyrocketed in the past 2-3 years. Rather, the real killers are the drugs that replaced the pills. (See: No, Vicodin Is Not The Real Killer In The Opioid Crisis ). Yet that hasn't stopped the agency from sticking to its mindless and simplistic plan of cracking down on the number of prescribed pills and, perhaps worse, setting guidelines that define a fixed daily limit on dose. This was all but guaranteed to accomplish little except causing needless suffering, which is just beginning to become evident. From the CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016:
"When opioids are started, clinicians should prescribe the lowest effective dosage. Clinicians should use caution when prescribing opioids at any dosage, should carefully reassess evidence of individual benefits and risks when considering increasing dosage to ≥50 morphine milligram equivalents (MME)/day (1), and should avoid increasing dosage to ≥90 MME/day or carefully justify a decision to titrate dosage to ≥90 MME/day."
Source: CDC Guideline for Prescribing Opioids for Chronic Pain — United States, 2016
What a mess. And we are seeing just the beginning of how much suffering will result from this foolhardy policy. For example, Maine passed a law that ensured that an 81-year-old woman with psoriatic arthritis will not be able to sleep through the night (emphasis mine) (2):
Jane Avery says the pain from her psoriatic arthritis is the worst at 2 a.m. when she can't sleep and already has met her daily limit on painkillers. Her daily dosage of the drugs was cut in half about six months ago... [B]y July, Maine doctors will not be allowed to prescribe more than 100 milligrams of opioid medication per day to most of their patients.
Source: US News and World Report - "Chronic Pain Patients Say Opioid Law Creates New Crisis" Disgraceful
There are plenty of other Janes out there, and their lives are about to get much worse. This one-size-fits-all approach regarding opioid dosage can't work. People are just too different in how their bodies handle opioids, which is precisely the conclusion of a 2012 article in Medscape Medical News entitled "Need for High Opioid Dose Linked to CYP450."
The essence of the article is that some patients, through no fault of their own, require much higher doses of opioids than others to relieve their pain. This cannot be more clear:
"We've known for years that among patients with the exact same pain conditions one may need 500 mg of morphine a day while the other may need only 50 mg, but we've always wondered why.
Forest Tennant, M.D. Medscape Medical News
Here's why: It's all in the genes.
"It turns out that among high-dose patients, about 85% have these defects in 1 or more of their CYP450 enzymes. In the general population, only about 20% to 30% of people have CYP450 defects."
The two sentences above tell us why the CDC-recommended dose of 90 MME is so ridiculous, and why pain sufferers like Jane Avery can't sleep at night. Pain patients who are taking high doses of opioids are not doing so because they just happen to feel like it. No—they are often people who have abnormal liver enzymes, which make their livers especially efficient at metabolizing the very drugs they need to control their pain.
So, let's give the CDC an F for policy, only because there is no lower grade. But the agency managed to get the science wrong as well, which is one of many reasons there will be many more Jane Averys with time. Let's give them an F for science as well.
Perhaps they should have called on a medicinal chemist. Any one of us could have seen this coming a mile away because it's one of the maddening problems that plagues those of us who do drug discovery research. It is called ADMET.
ADMET is short for Absorption, Distribution, Metabolism, Excretion, and Toxicity. Drugs live or die because of ADMET, and all five of these properties of any given drug are difficult to predict in advance. As a result, many experimental drugs have met with an early demise when a failure of even one of these properties turns an otherwise promising molecule into something that ends up in a waste disposal container (2).
This is where the CDC really got it wrong. The agency failed to take into account ADMET (3) when making its recommendations. The one-size-fits-all dose that is supposed to keep pain patients from becoming addicted (4) is really one-size-fits-none.
Let's focus on the metabolism component of ADMET, since it is metabolism that speaks directly to the practice of defining a fixed doses of opioids. It is well known that there are substantial differences in the rate (and type) of metabolism of a drug from species to species. But there can also be substantial individual differences, even within any one species, such as humans. This variability makes an already tough job—defining an appropriate dose—even tougher. While most people who take drugs will fit within a reasonably narrow range of blood levels per given dose, some do not. These distinctions arise from both the quantity and composition of ubiquitous liver enzymes called CYPs (short for cytochrome P450). They are the primary drivers of drug metabolism and excretion.
Perhaps the quintessential example of consequences of the genetic variability of CYP enzymes is the profound difference in how many Asian people respond to alcohol. (See: Alcohol is Racist. Unhappy New Year For Some). Asians are far more likely to have a deficiency in the CYP gene that produces an enzyme called acetaldehyde dehydrogenase (ALDH). ALDH is responsible for the second step of the two-step process in the metabolism alcohol. When both steps are working properly, alcohol is converted into harmless acetic acid. But when ALDH is not present or functioning properly, acetaldehyde—the product of the first metabolic step—builds up in the blood. Acetaldehyde is quite toxic, and this genetic difference alone is sufficient to prevent some Asian people from being able to tolerate even small amounts of alcohol (5).
A different gene called CYP2D6 is responsible for the metabolism of most opioids (6), and CYP2D6 displays quite a bit of what is called genetic polymorphism (small variations of the same gene). These seemingly small differences in this single gene can nonetheless play a very large part in the wide range of responses opioids in different individuals. Within a given population, there can be as much as 15-fold differences in metabolism between those who are poor metabolizers, and those who are very good (7). The meaning of Dr. Tennant's quote (above) should now be obvious.
The genetic component of opioid metabolism differences is further examined in a paper from the journal Clinical Pharmacology & Therapeutics. "Worldwide Distribution of Cytochrome P450 Alleles: A Meta-analysis of Population-scale Sequencing Projects" provides a very detailed discussion of genetic polymorphisms in the CYP genes. The paper is some pretty rough going, but there is a take-home message: "single nucleotide variants and copy number variations in CYP genes are major determinants of drug pharmacokinetics and toxicity and constitute pharmacogenetic biomarkers for drug dosing, efficacy, and safety." In other words, seemingly-small genetic differences between individuals can have a significant impact on how people metabolize drugs.
So, perhaps the high and mighty who have made the recommendations and regulations that treat pain patients, who need large doses of opioids just to survive as moral degenerates, may want to reconsider their judgmental thinking and "guidelines." Because an arbitrary maximum dose of an opioid is tantamount to torture of the unfortunate people who did nothing wrong except be born with defective CYP genes. Instead of treating them like lepers, perhaps we should pay attention to the science. Or maybe this is far too much to ask of the CDC, whose policies are causing needless suffering while at the same time doing nothing to change the number of opioid overdoses, except increase it. (See: "No, Vicodin Is Not The Real Killer In The Opioid Crisis.")
Bad policy based on bad science. Our government at its worst.
Notes:
(1) Morphine milligram equivalents (MME) is an approximation of the strength of a dose when related to morphine as a standard. Since different opioids have different potency, the MME will be different for many of them. For example, 90 MME is the same as 90 mg of Vicodin (nine 10 mg pills) and 60 mg of Percocet (six pills). Many chronic pain patients have been taking far higher doses for years.
(2) In the 1990s at Wyeth, I was running an antiviral program looking for new therapies for three different herpesviruses. Everything looked great until three years into the program—just before we intended to start Phase I clinical trials— we discovered that a series of highly potent inhibitors of cytomegalovirus (CMV), herpes simplex, (HSV) and varicella/zoster (VZV), which looked fantastic in in vitro assays, and were well absorbed and stable in three different species of animals, fell apart very rapidly when exposed to human liver cells. Instead of a clinical candidate, we had on our hands three years worth of useless chemicals. This really sucked.
(3) Differences in metabolism are not the only factor that makes standardized dosing of opioid a scientific abomination. There are also individual differences in the responses of the brain to the drug, which are independent of metabolism. Just one more reason that makes the fixed dose approach so flawed. This discussion is beyond the scope of this article.
(4) In reality, very few pain patients who take even high-dose opioids become addicted. Those who become addicted are usually recreational users.
(5) There is a drug called Antabuse, which is used to prevent alcoholics from drinking. Antabuse blocks the action of acetaldehyde dehydrogenase. Anyone who is taking this drug will become violently ill from even a single sip of alcohol.
(6) Table 1: The primary CYPs of opioid metabolism.
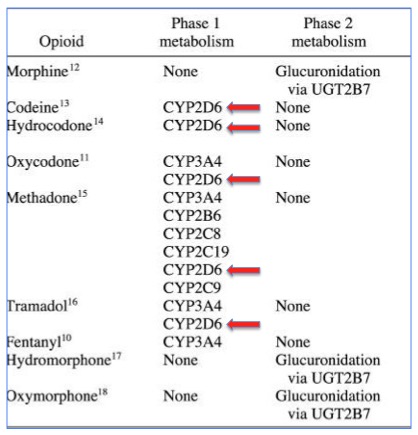
Source: Mayo Clin Proc. 2009 Jul; 84(7): 613–624. Note that CYP2D6 is responsible for the metabolism of most opioids.
(7) There are 74 known subtypes of the CYP2D6 gene in humans.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


