Dr. Leejee H. Suh, an Associate Professor of Ophthalmology at Columbia University Medical Center in New York, kindly took the time to answer some questions about corrective lens implantation, a painless and remarkably effective method of vision correction, which can correct two problems, cataracts and farsightedness or nearsightedness, in less than one-half hour. Although the technique is not new, I had no idea of what to expect, even though I write about science and medicine (1). To the patient, it must seem more like magic than medicine. The results are that striking.
JB: Dr. Suh, thank you for taking the time to speak with me. I am sure that many of our readers either do not know or don't fully appreciate the power of the techniques that you use. Can you tell us a bit about cataracts, and how they impact vision?
LS: A cataract is when your normally transparent lens becomes cloudy and so the vision becomes compromised. Symptoms of cataract are increased glare or light sensitivity particularly with night driving, overall blurry vision, diminished contrast.
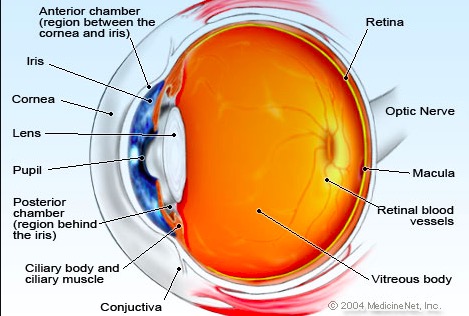
The anatomy of the eye. Graphic: MedicineNet
JB: When were lens replacements first used to treat cataracts? Can you compare the techniques used earlier to those that you use today?
LS: Although cataract surgery (or removal of cataracts) is one of the earliest documented surgeries (5th century BC), its recent advancements have made it one of the most successful types of surgery around. In the late 1940s, a British ophthalmologist Dr. Harold Ridley recognized that plastic in the eyes of injured WWII soldiers remained inert and so created the first intraocular lens (IOLs) in 1949. In 1967, a New York-based ophthalmologist, Dr. Charles Kelman, introduced phacoemulsification surgery in which ultrasound energy is used to cut the cataract and then the pieces are vacuumed out of the eye through a small incision.
With this technology, foldable lenses were developed so that the plastic IOLs could go into the eye through a smaller incision. From then on IOLshave come a long way. More recently in the last 10-15 years, specialty IOLs have changed the face of cataract surgery, where before it was to just improve vision from non-seeing to seeing to now as a "refractive" procedure in which vision is improved to levels better than before surgery.
JB: Most of have never heard of a toric lens. How is it different from other lenses?
LS: A toric intraocular lens helps correct corneal astigmatism that a standard monofocal lens will not. Astigmatism is a property of the cornea's shape that causes an image to be blurred without proper correction via spectacles or contact lenses. The utility of implanting a toric IOL in someone with corneal astigmatism is that their image without the aid of spectacles or contacts will be clearer.
JB: Most people get rather queasy when thinking about anything touching their eyes, let alone cutting into them. Yet, I felt nothing, even though I was awake, Can you describe how the drugs that are used numb both the eye and the patient?
LS: All patients who undergo cataract surgery receive some level of monitored anesthesia care (MAC sedation) so they are less anxious and then also receive anesthesia topically (eyedrops) and intracamerally (into the anterior chamber of the eye). With these levels of anesthesia, almost all patients are comfortable.
JB: When people hear the word "surgery," they reflexively think of hip replacements or appendectomies. But the lens implant is a type of surgery, albeit a very delicate one. The precision required for this type of procedure may be impossible for us to grasp. Can you describe the techniques that are used to ensure such precision?
LS: Cataract surgery is microsurgery where incisions are in the millimeter range. It is also a very dynamic and bloodless surgery in which fluid is removed and replaced throughout the procedure. The steps of modern day cataract surgery are:
- A small incision is made in the cornea; a small circular cut is made in the anterior capsule of the lens; the nucleus and cortex of the lens are removed with the phacoemulsification unit;
- The lens capsule is left intact into which an intraocular lens implant is placed; the corneal wound is then self-sealing with the placement of some fluid in the wound (hydration).
JB: Replacement of a cloudy lens with a clear one seems straightforward enough. But combining this with vision correction is much less so. Can you tell us how you determine the amount of correction needed, how this information can be used to select the replacement lens, and how it is implanted with such precision?
LS: Cataract surgery is the removal of the cataract with a placement of a new intraocular lens. The power of the selected IOL determines the refractive power of the eye (farsightedness, nearsightedness, astigmatism). The power of the IOL is determined with eye measurements that the patient receives in the preoperative assessment. The surgeon then discusses with the patient his/her visual needs to determine what IOL to place in the patient's eye, for example how they want to see after surgery without glasses. There are four different types of IOLs available to patients-- standard monofocal IOL (gives either distance or near vision without astigmatism correction), toric monofocal IOL (gives either distance or near vision with astigmatism correction), multifocal IOL (gives a range of vision from distance to near without astigmatism correction) and toric multifocal IOL (gives a range of vision from distance to near with astigmatism correction).
JB: What can go wrong? What is the incidence of complications? How serious can they be?
LS: Modern day cataract surgery is one of the most successful types of surgery in general (>95%). Complications are extremely rare but include infection, inflammation, transient elevation in eye pressure, retinal complications. Most of all the potential complications can be addressed in the postoperative period.
NOTES:
(1) Dr. Suh performed two lens replacements on me, one this past April and the other in early November.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


