US news media headlines appear daily on the so-called “opioid crisis”. A major thread in public policy discussions is an asserted need to “solve” the crisis by limiting production of opioid analgesics and reducing medical exposure to potentially addicting drugs. But are such steps actually a remedy? Will US addiction and overdose problems respond favorably to such a one-size-fits-all policy? Almost certainly not.
A recent analysis has been performed on data downloaded from the US Centers for Disease Control and Prevention and the US Agency for Healthcare Research Quality (1). The data characterize medical opioid prescribing, opioid overdose-related deaths from legal and illegal drugs and hospital emergency room admissions from 1999 to 2016 for 50 US States and District of Columbia. Figure 1 is constructed from the most recent CDC data.
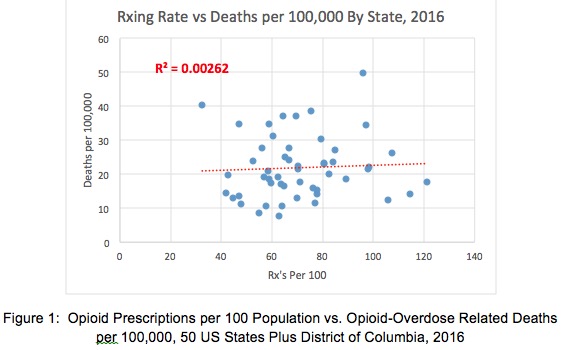
Two insights emerge:
- There were major variations but no trends in opioid OD death rates and opioid prescription rates from State to State in 2016.
- Opioid OD death rates had no apparent relationship to opioid prescription rates from State to State. Any effect of medical prescribing on OD deaths was literally “lost in the noise” of other factors.
Examination of individual US States reinforces these insights. Table 1 compares CDC and AHRQ data on opioid prescribing and overdose-related deaths for five US States and the District of Columbia. California, New York, and Florida have high populations. Massachusetts and Oklahoma are less populous. Oklahoma has the second highest opioid prescription rate, while the District of Columbia has the lowest prescription rate in the US.

Overall risk of opioid-overdose-related death in the US was about 0.015% per year, with State rates between 0.01% and 0.025% in 2016. District of Columbia, with a population of ~575,000, had the lowest rate of opioid prescribing, but consistently higher opioid-OD related death rates than New York (population ~19 Million) or California (~33.5 Million).
As prescribing rates for medical opioids fell in 2010-2016, opioid OD-related death rates continued to climb. However, the shape of growth curves is quite different for DC, Massachusetts, Florida and New York (each with sharp upward trends in death rates for 2015 and 2016) versus Oklahoma and California (which remained relatively stable).
California OD-related death rates edged upward by 18% from 2006 to 2016, while death rates doubled in New York. In both States, rates of emergency room visits rose by about 270%. However, opioid prescription rates in California dropped by 13% while rates in New York were unchanged. (2)
These State to State outcomes suggest that the US is dealing with not one National opioid crisis but many local crises. In 2016, medical prescribing contributed almost nothing to these crises.
NOTE:
(1) Richard A. Lawhern, Ph.D., “US Opioid Prescribing vs. Overdose Deaths and Hospital ER Visits -- Implications for Public Policy,” Alliance for the Treatment of Intractable Pain, April 2018. Original data download and initial graphical analysis performed by John Alan Tucker, Ph.D., used with permission. http://www.atipusa.org
(2) Emergency room visit data downloaded from Agency for Healthcare Research Quality (AHRQ) HCUP database, current December 2017; latest year available for the selected States was 2015.