
Aortic stenosis refers to a narrowing of the valve leading from the heart to the aorta supplying oxygen and blood to the body. It simultaneously robs the body of these necessities and increases the strain on the heart as it pumps harder and harder against fixed narrowing. Medicine has converted it from a death sentence with the development of open, surgical repair or replacement of the aortic valve (SAVR) and in the last few years that benefit has been extended to the increasingly frail and higher-risk patient through a minimally invasive technique, transcatheter aortic valve replacement (TAVR). TAVR can replace the valve without the need for a sternotomy, “cracking the chest,” opening up the breast bone to get at the problem.
The results with TAVR are improving all the time, and the procedure is moving from being offered to only the high risk to those who might do as well with SAVR. A new paper in JAMA Internal Medicine reports on a comparison of those two approaches but what makes the paper important is both how they characterize the risks associated with frailty and how they describe the outcomes. They looked at 350, 70-year old or greater patients undergoing elective repair without a significant acute event prompting intervention. Treatment was not randomized by the study which simply was an observational study of outcomes.
Frailty
Frailty is more than just the risk factors like lung or kidney problems. It is countless other factors, how much a patient’s glucose metabolism is impaired, their muscle strength in gripping your hand or walking quickly 15 or 20 feet. The first innovation of the paper is to characterize patient frailty using an index that takes into account many of these factors in a yes/no way; for example, there is no need to describe how abnormal a HgA1c is, just being elevated is sufficient for this scoring. And then you can also count activities of daily living, like whether the patient can get up and get dress and feed themselves without assistance. This scoring method has been shown to be an excellent predictor of frailty across many diseases. As abnormalities increase the frailty index rises, to a maximum of 1, representing all the measures; in reality, few individuals are alive when their frailty index is .6 or higher, when 60% of the measures are positive.
Outcomes
Typically outcome is based on whether the patient is dead or alive and whether the treatment “fixed” the problem, in this case, improved heart function. And most studies have shown that in one month, TAVR and SAVR are both very good at fixing the problem. But in this study outcome was characterized by how patient’s functional abilities, measured by 22 acts of daily living and simple physical tasks, e.g., carrying groceries, changed from pre-procedure to 1 year later – were their lives better?
Here is the 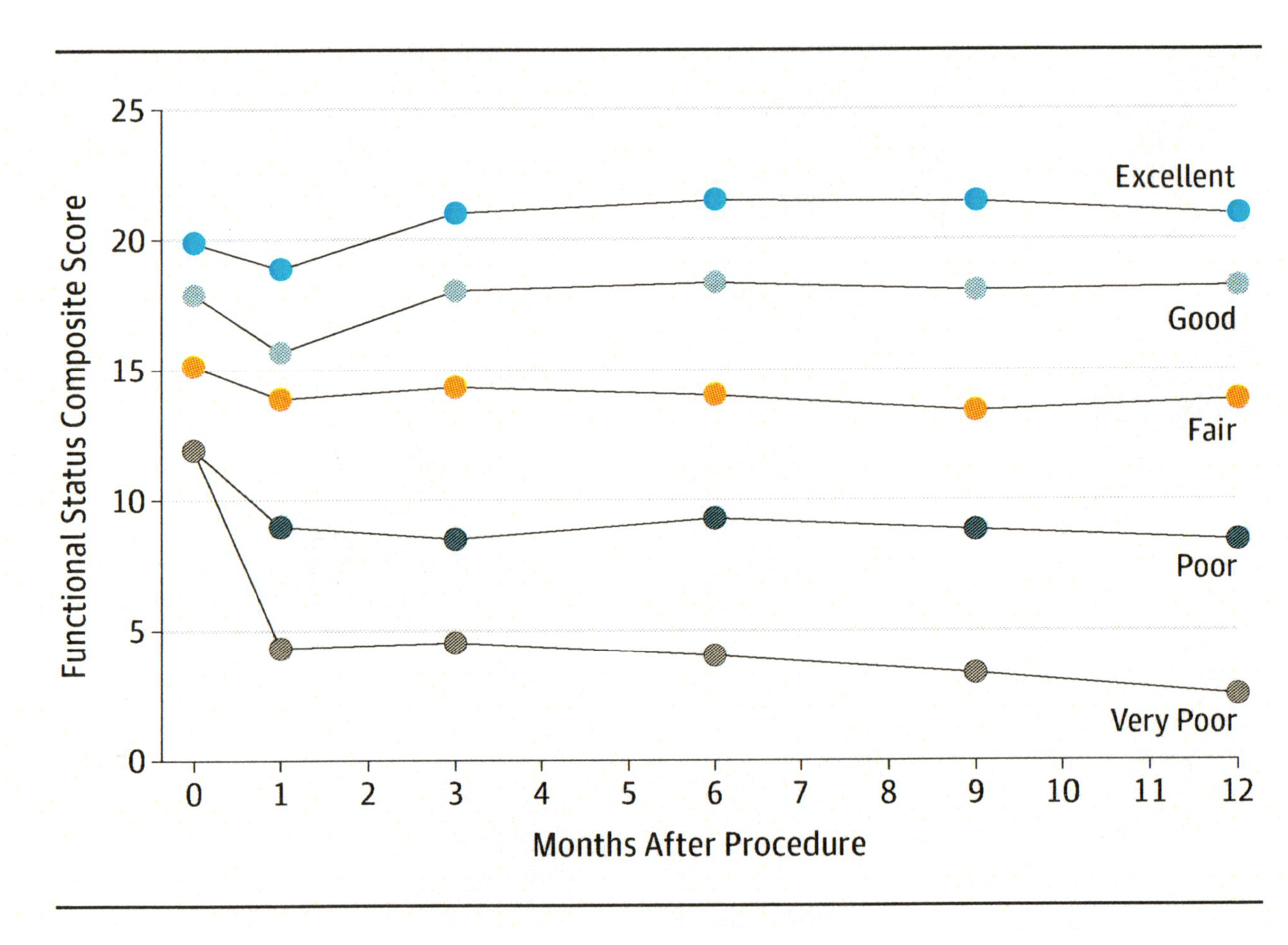 graph that identified five patterns of recovery. In each case everyone’s functional ability declined at one month, no surprise, everyone was still recovering from their procedures. But look at the degree of decline, especially for those who were functionally impaired pre-operatively, they had significant drops. Look at the recovery at one year; only two groups were improved or stayed the same, the others declined. And before going further there is no control to show the decline in function for those not treated with TAVR or SAVR, so we needn’t jump to conclusions about the benefits or declines these procedures provide.
graph that identified five patterns of recovery. In each case everyone’s functional ability declined at one month, no surprise, everyone was still recovering from their procedures. But look at the degree of decline, especially for those who were functionally impaired pre-operatively, they had significant drops. Look at the recovery at one year; only two groups were improved or stayed the same, the others declined. And before going further there is no control to show the decline in function for those not treated with TAVR or SAVR, so we needn’t jump to conclusions about the benefits or declines these procedures provide.
When looking at these outcomes, the improvement in a patient’s life is more muted and attenuated than the improvement to heart function. For TAVR, offered to the higher risk and frail, about a third of patients improved and a quarter of patients declined, and the rest remained unchanged. For SAVR, three-quarters improved, with only a few declining. The frailty index tracked with these more general, dare I say, important functional life outcomes.
Precision medicine
For physicians counseling patients, this opens up an important component to the discussion. As the paper suggests, half of the patients with a frailty index of more than .5 or 50% functional abnormalities can successfully undergo TAVR, escaping complications and having significant improvement in their overall heart function. But there is virtually no chance for functional improvement, their life will be no better, and there is a “good chance” that they will be placed in a nursing home. We can now provide better information about functional outcomes and the road patients must travel to get them.
Similar data exists or can be developed from a variety of medical interventions. Isn’t time to begin discussing not just whether surgery or medical treatment will cure or what its side effect or complications might be, and start to share how well the patient, the one sitting in front of us, will recover and how much better or not they will be? That is real, patient-focused, precision medicine that we can provide now.
Source: Evaluation of Changes in Functional Status in the Year After Aortic Valve Replacement JAMA Internal Medicine DOI: 10.1001/jamainternmed.2018.6738

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


