“The hygiene hypothesis suggests that our immune system works best when it has been exposed to a diversity of foreign others and that population measures of hygiene, such as running water, waste disposal systems have not so much weakened as altered our responses.”
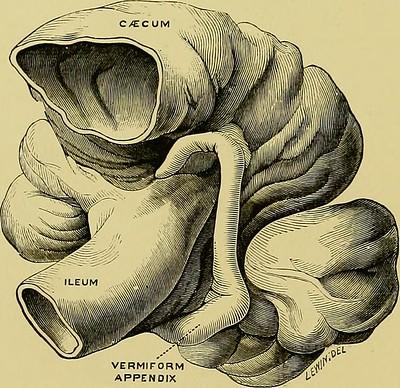
The appendix is an outpouching at the very beginning of the large intestine, in an area called the cecum. It is of variable length, but its internal diameter is relatively small and constant. It contains a great deal of “lymphoid tissue,” a component of our immune system, like lymph nodes, harboring white blood cells. Most cases of appendicitis in Western, high hygiene, countries, are felt to be due to this lymphoid tissue enlarging, closing off the small lumen of the appendix. Subsequently, the mucous created within the appendix causes pressure to build, cutting off the appendiceal blood supply. The death of the appendix results in spillage of the large intestine contents, bacteria, and feces, throughout the abdomen.
Untreated appendicitis is lethal, with mortality that approached 85%. Surgical and medical management have significantly reduced this number to roughly 0.4%, mainly due to the effects of the spillage of a burst appendix. But we digress.
The key here is mucous, that slippery fluid more often associated with a runny nose. But mucus serves many masters, capturing large dust particles from entering our lungs to providing a protective barrier where bacteria can hide and hang out. Mucous, which in this instance is termed a biofilm, acts as a “safe house” for bacteria allowing them to escape from other bacterial predators, and antibiotic assault. As it turns out, the appendix has the highest concentration of these biofilms throughout the large intestine. These biofilms do not cling inside the appendix forever but are continuously shed, along with their bacterial contents downriver, so to speak, through the large intestine. Finally, the position of the appendix at the beginning of the large intestine, and its small opening afford it protection from bacterial invaders both in the fecal stream or that have arrived from oral intake.
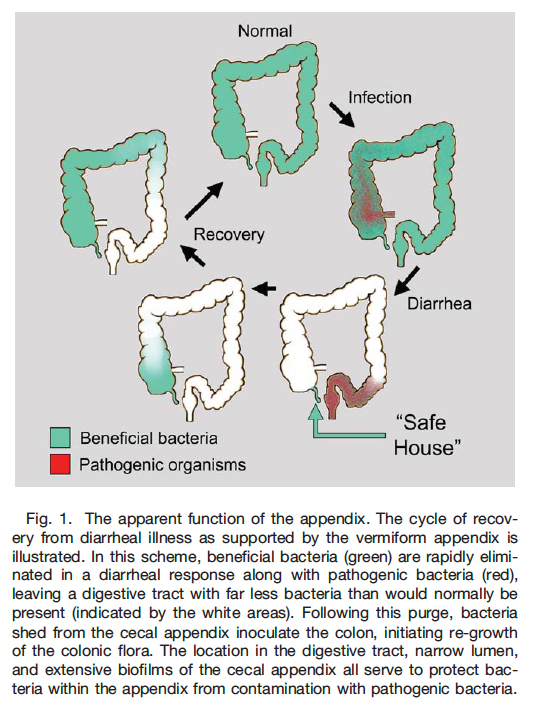 Taken all together, the belief is that the appendix serves to replenish the gut with its normal microbiome after undergoing infection by a pathogen. This is especially true for diarrheal diseases, often secondary to untreated drinking water, the type of conditions that kill many children in low hygiene countries. Diarrhea rapidly removed bacteria, good and bad, from the large intestine, resulting in the removal of the pathogen, but at the same time depletion of the normal bacterial microbiome. It is believed that the appendix holds the inventory of our normal flora, releasing it back to repopulate the large bowel’s microbiome.
Taken all together, the belief is that the appendix serves to replenish the gut with its normal microbiome after undergoing infection by a pathogen. This is especially true for diarrheal diseases, often secondary to untreated drinking water, the type of conditions that kill many children in low hygiene countries. Diarrhea rapidly removed bacteria, good and bad, from the large intestine, resulting in the removal of the pathogen, but at the same time depletion of the normal bacterial microbiome. It is believed that the appendix holds the inventory of our normal flora, releasing it back to repopulate the large bowel’s microbiome.
Appendicitis is about 35 times more common in high hygiene countries as compared to those with low hygiene. And as the sanitation in these countries rises, so does the incidence of appendicitis.
‘‘When we come to realize how slowly evolutionary processes have affected man’s body in past times, we can hardly expect our internal digestive system to adapt itself to the rapid pace demanded by the ever-accumulating resources of civilization.’’
The hygiene hypothesis suggests that there is a mismatch between an immune system that developed over millions of years and the very recent improvements in hygiene. By that, I mean a reliable source of clean water and separated waste streams – changes that are roughly 100 to 150 years old.
All of this leads to an illustration of the meaning of “fitness” in evolution. In highly industrialized, hygienic countries, the loss of the appendix is of little apparent consequence; 5% of the population has had theirs surgically removed. For us, the appendix is more a disaster waiting to happen, or revenue enhancement, than an improvement in our fitness to survive. But for countries with water and food-borne gastrointestinal illness, the appendix continues its evolutionary role, restoring the microbiome after a diarrheal illness has swept everything away.
Much of this is not proven, and for a variety of ethical and logistical reasons, it is doubtful that a human study will be undertaken. But it does point out that “fitness” is not absolute, but contextual; it again raises the intriguing notion that our physical and societal evolutions are out of sync with one another.
“Given a wide range of observations from medical science, evolutionary biology, immunology, and comparative anatomy described above, it seems likely that the appendix, like other components of the immune system designed to fight threats that no longer apply to many humans, is not only made obsolete by factors associated with post-industrialized culture, but is overly reactive or sensitive due to an absence of stimulation.”
Source: The Cecal Appendix: One more Immune Component With A Function Disturbed By Post-Industrial Culture The Anatomical Record DOI: 10.1002/ar.21357

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


