
While there is no consensus on the number of primary physicians and specialists that are needed, most expert opinion believes that there is a shortage, that will grow with our aging populations. In the US, the estimates are for about a 120,000 shortfall in the next decade; globally, that number rises to 2.8 million. In both the US and the UK, about a quarter of the physicians are immigrants. While I could not identify a more detail evaluation for the US, in the UK, nearly 75% of those physicians come from low and middle-income countries (LMIC).
The physician brain-drain is alive and well and was the subject of a study reported in the British Medical Journal. While previous studies have focused on the money lost to LMICs in educating physicians, the researcher here focused on the cost to the population left behind in terms of poorer health outcomes. While the loss of life is “modest,” if one can use that word in this setting, highest in Africa at 1.72 lives/year/physician lost, using cost as the outcome produces larger numbers and, unfortunately, wider confidence intervals. [1]
To determine cost, the researchers used a simple formula. The value of a life multiplied by the number of lives a physician can save multiplied by the number of physicians migrating. Unfortunately, the straightforward equation’s terms are fuzzy. There are several ways to calculate the value of a statistical life. It is an economic valuation, what life means to the economy, not to the individual or family. In the US, it is put at about $10 million, but the value changes based on the country’s economy, and for LMICs, the valuation is less. The valuation of life also decreases with age; the choice of maternal and early childhood mortality as the measure of lives at risk is appropriate for the LMICs, but it keeps that valuation at the upper bounds, once again a bigger number.
Finally, the number of physicians migrating comes from governmental sources. [2] That number varies with geography, being highest from Africa (11.3%) and lowest from the Western Pacific (0.9%). The migration is inversely related to income, greatest from the low-income countries (11.07%), then low-middle income countries (6.29%), and 2.66% from middle-income countries. Here is the graphic.
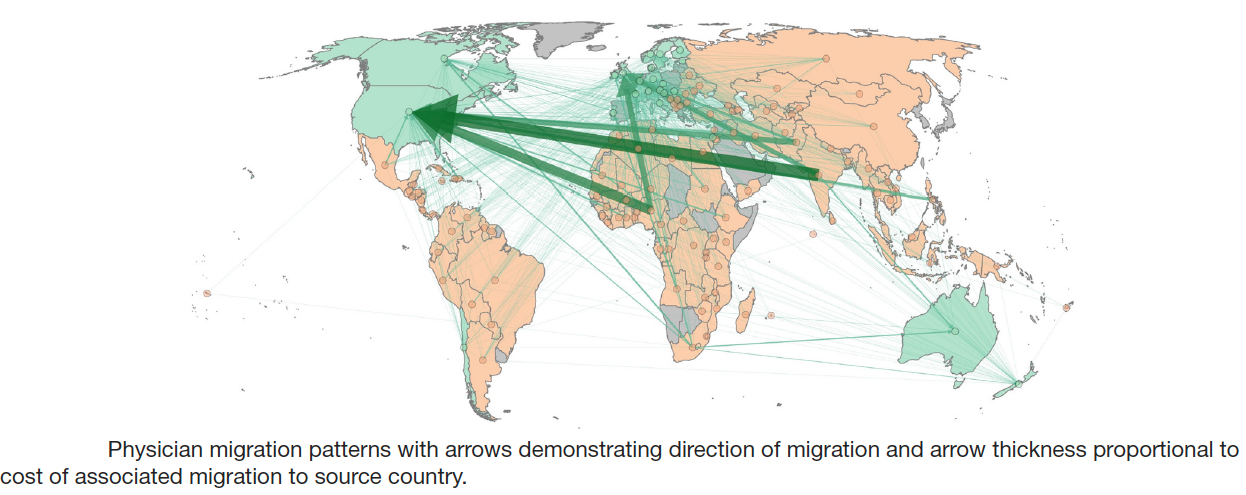
3.9% of the physicians trained in LMICs currently practice in high-income countries
As we would expect from the formula, most of the “cost” is from the value of those lost lives, especially those childhood deaths. [3] The highest total costs accrue to India, Pakistan, Nigeria, and South Africa. If you relate costs to the country’s gross national income, then the biggest losers are the people of the Congo, Ghana, Liberia, and Sierra Leone.
The bottom line, those countries that can least afford to lose physicians see them leaving for high-income countries. If you are one for metrics, the performance of the foreign medical graduates (FMGs) in the US is as good or better than the home educated; so in some ways, we are taking everyone’s “best and brightest.” While we cannot determine why the physicians migrate, the pursuit of a better life, resources, and income are surely in the mix.
We can pull apart the researchers’ calculations on several grounds; they are the first to admit the uncertainty of the inputs. But the value of the exercise lies in shifting the conversation from the money lost educating a physician, to the lives lost year after year when there is no replacement for that physician. It is interesting to conjecture whether the push for nurse practitioners to fill the primary care shortfall would be useful, as well, in these LMICs.
[1] This is an excellent example of choosing an outcome that will garner more attention, publication bias.
[2] A migrating physician is one who receives their training in an LMIC country and practices in a high-income country.
[3] Maternal deaths have a smaller cost because mothers have lived longer.
Source: The impact of physician migration on mortality in low and middle-income countries: an economic modeling study BMJ Global Health DOI: 10.1136/bmjgh-2019-001535

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


