As with most viral infections, the standard treatment, and this applies to roughly 80% of Covid-19 cases in the aggregate population, is rest, hydration, and symptomatic relief, i.e., antipyretics – medications to reduce fever and antitussives – medications to reduce coughing. But knowing your Covid-19 status means that you can be appropriately quarantined and treated in your home or hospital.
In a world of limited resources, and that is the current case with Covid-19 testing, more plentiful tests for seasonal flu and bacterial sources of infections are employed to screen out these causes and concentrate Covid-19 testing on more likely individuals. The data so far indicate that as with all testing, there is a percentage of false negatives, meaning the test shows no evidence of Covid-19, but you are still infected. For that reason, in the face of an initial “negative” result, an additional test performed 24 hours later is required to be assured that no infection is present. For symptomatic patients, those with an elevated temperature and/or a dry cough, two tests will be necessary, because those symptoms heighten the probability of you being infected. In a setting of rationing tests, one negative test may have to do if you are otherwise asymptomatic. Because we are attempting to slow the person-to-person spread of Covid-19, social contact with a confirmed Covid-19 patient will result in testing.
Home or Hospital
Once you have been deemed infected, you are at risk of passing the infection on to those around you. The majority of Covid-19 positive individuals can be treated and quarantined at home – reducing an increasingly stressed health system. Hospitalization is confined to those patients at increased risk of complications, the primary one being respiratory. The key symptomatic trigger will be shortness of breath. These individuals need to have their ability to oxygenate blood monitored, and that is most safely done in a hospital setting. Other individuals at higher risk, specifically the immunocompromised, may be admitted out of an abundance of caution. However, caution will take a backseat to shortness of breath when we need to triage beds due to lack of capacity.
Med-Surg or Intensive Care
As with any illness, placement in the hospital is based on the acuity of need. The severely ill are placed in areas with a higher nurse to patient ratios [1], better monitoring, and the ability to apply more invasive care – intensive care units. The walking wounded are placed where there is supportive care and routine surveillance – medical-surgical units. And there are additional, “step-down” units providing intermediary care, less than ICU, more than med-surg, designed to transition patients between these two levels of care. In step-down units, once again, nursing to patient ratios are slightly higher and more sophisticated, but not necessarily invasive care is available, primarily because there is the support staff to monitor that care.
Since the majority of deaths from Covid-19 have a respiratory cause, your ability to oxygenate, get oxygen to the tissue, is the crucial sign monitored [2]. As our ability to absorb oxygen into our bloodstream declines, our lungs respond by increasing the rate of breathing and increasing the expansion of the lungs to take in more air; making greater use of our respiratory and accessory muscles to increase the expansion of the lungs taking in more air [3]. The ability to absorb oxygen into the blood is measured by a pulse oximeter, a small device attached to your finger that uses light to measure oxygen levels. In many instances, supplemental oxygen will be sufficient to tide one over as they recover, but for patients with pre-existing respiratory conditions, this may be insufficient. At some point, they can no longer sustain the additional work of expanding their lungs and increasing the rate of breathing; they tire out, and the mechanics of inhaling, exhaling, and oxygenation fail.
In these circumstances, breathing needs to be assisted, and a mechanical ventilator takes over the work of breathing and providing supplemental oxygen while your body recovers. The most effective way to couple your lungs with a ventilator involves placing an “endotracheal tube” in your trachea, the entrance to the lungs. These tubes are uncomfortable, and patients being mechanically ventilated will often be sedated, allowing them to “sleep through” the experience. In general, at this point, you are on life support requiring close monitoring of not only your vital signs, oxygenation and your level of consciousness, but the functioning of the ventilators (which are well-tested, safe systems) as well.
Mortality
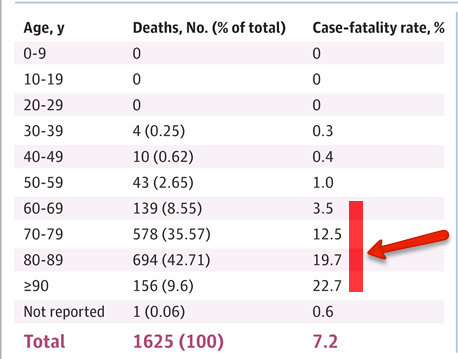 There is no specific treatment for Covid-19; care is supportive. Death is related frequently to your resilience, in a positive manner, or frailty, with a negative association. [4] Public officials are indicating that the age group at risk are those over 60 years of age. But this is not a homogenous group, some members are fit, others spry, and some are frail. Here is the most current data from Italy, the over 60s are highlighted. Age is a shorthand to describe the group. Take the numbers as a rough gauge, not hard and fast. Within any of these age group, mortality rises with frailty, especially cardiopulmonary debility; the percentage of the population that is frail increases with age
There is no specific treatment for Covid-19; care is supportive. Death is related frequently to your resilience, in a positive manner, or frailty, with a negative association. [4] Public officials are indicating that the age group at risk are those over 60 years of age. But this is not a homogenous group, some members are fit, others spry, and some are frail. Here is the most current data from Italy, the over 60s are highlighted. Age is a shorthand to describe the group. Take the numbers as a rough gauge, not hard and fast. Within any of these age group, mortality rises with frailty, especially cardiopulmonary debility; the percentage of the population that is frail increases with age
The idea of flattening the curve, spreading out the disease over time, is to allow for repurposing resources – where you are placed, who cares for you, and what monitoring and supportive care are needed. Alternative locations may be the easiest repurposing, especially for patients that simply need monitoring and supplemental oxygen. Who cares for you, reallocation of labor is already underway. For example, stopping elective surgery frees up nursing staff to temporarily provide bedside care, and can open up beds in the surgical recovery rooms to house more medical patients. Similarly, closing down outpatient services frees up nursing staff to help lower the nurse to patient ratio and heighten routine or stepdown surveillance. The essential bottleneck will be the availability of mechanical ventilators. The response by the government and private sector is to ramp up production. Our individual response is to protect ourselves, our families, and those most at risk. Handwashing and social distance – a new way of saying stay home, don’t gather in crowds, limit your exposure to others, and their exposure to you.
[1] The typical ratio in the ICU is one nurse for every two patients; the ratio is 1 to 4 or more for routine “floor” care.
[2] Symptoms are expressed by patients, “I have a headache, I feel dizzy, I have a cough,” while signs are objectively identified and measured, like heart rate, a rash, etc.
[3] Our respiratory muscles are those between our ribs, the meat we relish when we eat spareribs. Other accessory muscles, in the neck, assist by pulling our chest upward to increase the expansion of the chest.
[4] Some patients develop cytokine storm when your immune system becomes so hyperactive that it turns upon you. The resilience necessary to combat cytokine storm is found far more in the young than old, and far, far, less in the frail.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


