In addition to the first three groups reporting, the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) has obtained data from an additional six sites or collaborations.
The London School of Hygiene & Tropical Medicine (LSHTM)
- The adjusted risk of death (adjusted for age, gender, co-morbidities, and geographic location) rose from the previously determined 35% to 58%.
- The absolute case fatality rate for those under age 55 was unchanged; for other age groups, the B.1.1.7 virus increased deaths consistently, i.e., greater numbers in those most at risk for the original strain of COVID-19.
- Residence made a difference; the increase in B.1.1.7 attributable deaths was 143% in nursing homes, 53% for those living in the general population.
The Imperial College of London
- They measured differences in outcome two ways; based on case fatality rates and using a control group weighted to reflect the characteristics of individuals infected with B.1.1.7.
- They found no change from their initial analysis; B. 1.1.7 was 29 to 35% more likely to result in death than “normal” COVID-19.
Public Health England
- They looked at 92,207 B.1.1.7 cases along with a matched cohort.
- The odds of hospital admission were not significantly different for the variant
- In a retrospective review, patients were followed for one month after a positive test. Subsequently, more outcomes have become available for this cohort. B.1.1.7 increased mortality by 65%. This is the same percentage they reported previously
University of Exeter
- B.1.1.7 increased the risk of death by 70% in a sample size of roughly 55,000 matched pairs. This cohort was younger and less representative of the elderly.
Public Health Scotland
- One study found an increased risk of death of 8% and a 40% increase risk of death and hospitalization.
- In a second study, hospitalization with the B.1.1.7 variant increased 63%, deaths by 37%
COVID-19 Genomics UK (COG-UK) Consortium
- B.1.1.7 was felt to increased deaths by 9% and admission to the intensive care units by 15%.
- Women had significantly higher ICU admissions and deaths than men.
The report goes on to present data from several other sites and collaborations.
The Caveats
- First and this is most important – “the absolute risk of death per infection remains low.” For the UK the case fatality rate is about 3%, roughly the same as the US (Johns Hopkins COVID tracker)
- The numbers reported above are relative risks. They will always be greater than absolute risk.
- Those studies involving in-patients “did not identify evidence of increased disease severity, this is not incompatible with an overall increase in disease severity.” The finding of no increase in in-patient deaths is unchanged from their prior report. One might reasonably conclude that the increased deaths were among out-patients.
- As with much of our COVID data, there are lag times and missing case information that makes the data less confident or complete.
The Conclusion
"Based on these analyses, it is likely that infection with VOC B.1.1.7 is associated with an increased risk of hospitalisation and death compared to infection with non-VOC viruses."
As I wrote previously, SAGE quantifies what they mean by saying “realistic possibility.” Here is the graphic.
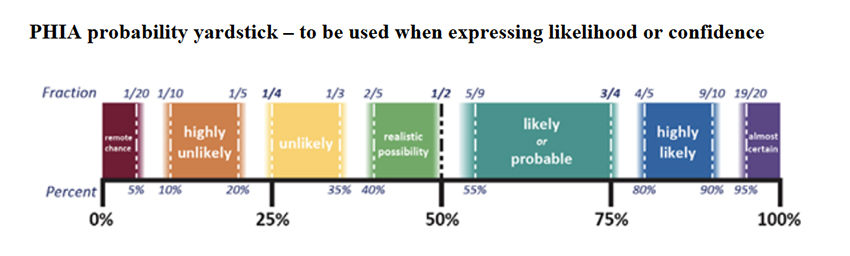
We are moving away from a 50-50 coin flip, and our belief that this variant is more deadly is growing but remains far from certain. "Likely or probable" remains a big range. We need time and more data, both of which require patience, another quality that we sorely need.
Source: NERVTAG note on B.1.1.7 severity New and Emerging Respiratory Virus Threats Advisory Group

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


