Back in April, I wrote about EIDD-2801, now called molnupiravir, (1) at which time I wrote "This drug seems to have a lot going for it." My opinion was based on the potent in vitro inhibition of SARS-CoV-2 as well as its ability to protect infected mice. Furthermore, molnupiravir inhibits the virus in a novel way called viral error catastrophe – inducing so many errors in RNA replication that the virus becomes so damaged just "gives up." (Given this property, it is not surprising that there was concern that the drug would be mutagenic (2), which is normally a giant red flag in drug discovery.)
Heather Boerner's article, "Five-Day Course of Oral Antiviral Appears to Stop SARS-CoV-2 in Its Tracks" in the March 9th Medscape discusses the latest Phase 2 data on the drug as well as some animal experiments. Following are some highlights and my comments.
"A single pill of the investigational drug molnupiravir taken twice a day for 5 days eliminated SARS-CoV-2 from the nasopharynx of 49 participants."
This is intriguing, but this doesn't tell us whether eliminating the virus from the nasopharynx (the upper part of the throat behind the nose) will impact the course or severity of COVID disease. Logically, it should, but "should" has been the downfall of many drugs.
"It has the potential to be practice-changing; it's not practice-changing at the moment." Carlos del Rio, MD, distinguished professor of medicine at Emory University.
Potential? Yes. Likelihood? Unknown. As you will see, molnupiravir is performing well so far, but there are unanswered questions. And, of course, it is a very big step from Phase 2 to Phase 3 and another from Phase 3 to approval. My colleague Dr. Alex Berezow has written a very helpful article, which explains the different phases of clinical trials.
Boerner discusses the Phase 2 study results. They are mixed. Patients with COVID-like symptoms (202) and a PCR confirmed infection were divided into three treated groups, each with different doses of the drug - 200 mg, 400 mg, and 800 mg. Placebo controls were used.
"By day 3, 28% of patients in the placebo arm had SARS-CoV-2 in their nasopharynx, compared to 20.4% of patients receiving any dose of molnupiravir. But by day 5, none of the participants receiving the active drug had evidence of SARS-CoV-2 in their nasopharynx. In comparison, 24% of people in the placebo arm still had detectable virus."
While this looks like nothing but good news there is a potential problem: "And although the reduction in SARS-CoV-2 was noticeable in the 200 mg and the 400 mg arms, it was only statistically significant in the 800 mg arm." There are a number of ways to interpret this statement:
- There were not enough patients to determine whether the drug works at the low and medium doses.
- In a larger trial, the 200 mg and 400 mg doses may show statistically significant viral reductions.
- It is possible that the minimum effective dose is 800 mg – a rather large dose.
- The numbers are shaky and the viral reduction seen in Phase 2 could disappear in a Phase 3 trial, where many more patients are tested.
Dr. Wendy Painter, the Chief Medical Officer of Ridgeback Biotherapeutics said "There's an urgent need for an easily produced, transported, stored, and administered antiviral drug against SARS-CoV-2."
Absolutely true. Although the vaccines are extraordinarily effective there are important reasons why we also need to add a pill to the COVID armamentarium.
- The pills are easy to make; much easier than a vaccine.
- They can be stored for long periods of time and don't need refrigeration – an important advantage in countries where refrigeration is not necessarily available.
- The drug might be effective against the emerging variants.
This is because molnupiravir doesn't have any effect on the spikes. Instead, it functions by disrupting RNA synthesis in the nucleus of the host cell, so molnupiravir could remain effective, regardless of the spike variants (3).
Bottom line
Molnupiravir has a pretty good chance of being approved, even if it is moderately effective in preventing severe COVID. It is considerably more potent than remdesivir in in vitro assays, and unlike remdesivir (which isn't used anymore), it can be swallowed instead of given IV, so it could be taken immediately after symptoms begin or a positive test. The safety profile looks good. And unlike remdesivir, the synthesis is easy.
Although there are some interesting experimental drugs (like Luvox) that seem to prevent severe disease, I'll take a direct-acting antiviral drug any day (4). Direct-acting antiviral drugs have made AIDS into a manageable condition rather than a death sentence, and now cure hepatitis C more than 95% of the time.
This would be a great drug to help tame the invisible monster that has plagued us for more than a year. Let's wish Ridgeback and Merck good luck in Phase 3 trials.
NOTES:
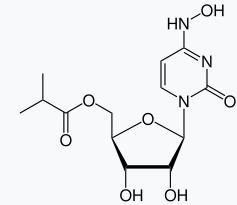
(1) The drug has a lot of names. The chemical name of active species is N-hydroxycytidine. It is also known are EIDD-1931 (EIDD is short for Emory Institute for Drug Development). To make matters more complicated, molnupiravir not EIDD-1931; it is a
(2) According to a press release from Merck (Ridgeback's partner) molnupiravir is not mutagenic.
Conference on Retroviruses and Opportunistic Infections 2021: Abstract SS777. Presented March 6, 2021.
(3) Of course, mutations of the virus at the site where molnupiravir acts that render the drug infective are also likely.
(4) Actually, I'll take two or more direct-acting antiviral drugs. AIDS and hepatitis C were tamed using cocktails, not single drugs. Resistance to single drugs will eventually (sometimes quickly) arise and the drug will no longer be effective. When two are more drugs that act by inhibiting different steps in viral replication it is much more difficult for the virus to become resistant.

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


