
The American Medical Association recently released a survey of 3,500 representative physicians on their “practice arrangements” - how they organize and pay themselves. Two or three graphs should tell our story.
Consolidation for size
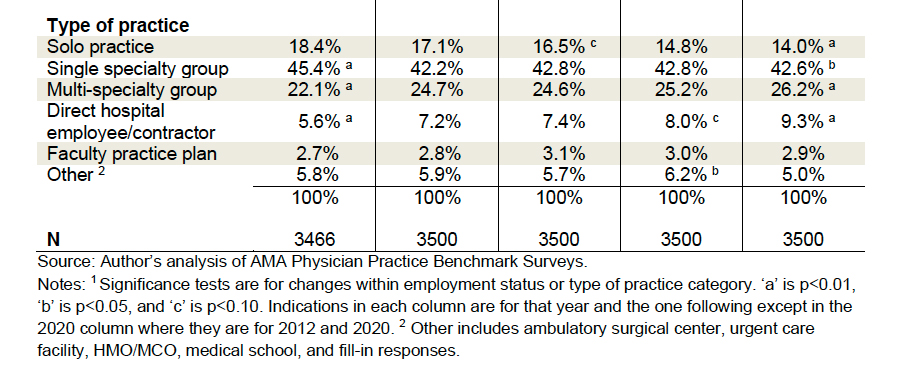 Solo practitioners, like pterodactyls looking for a tar pit, continue to decline, as do small 3-5 physician practices. Our “cottage days” of small practices are in retreat as practices must grow bigger to stay competitive and to negotiate with the shrinking pool of healthcare insurance carriers.
Solo practitioners, like pterodactyls looking for a tar pit, continue to decline, as do small 3-5 physician practices. Our “cottage days” of small practices are in retreat as practices must grow bigger to stay competitive and to negotiate with the shrinking pool of healthcare insurance carriers.
The demise of small office practices has many causes. With a majority of medical students borrowing money to complete their schooling and average debt in the range of $250,000, it takes at least a decade to pay it off. Many graduates do not have the financial wherewithal to finance setting up their own practice. The smaller the group, the more frequently the physician is on call at night or on weekends, taking time away from the life part of the work-life balance. Given the choice, I would join a larger group where I had more time off. Wouldn’t you?
Larger practices require more support services beyond billing, e.g., human resources coordinators, staff necessary to meet regulatory and quality data-gathering requirements, and IT staff to maintain the electronic health records and billing system. Few physicians are trained in these areas; fewer still can manage an extensive practice and practice medicine simultaneously, which gives rise to a layer of management.
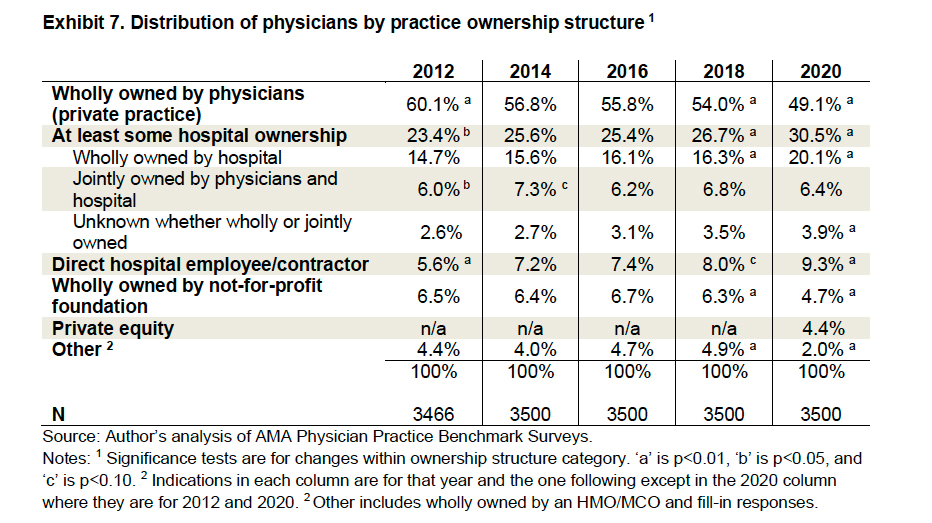 Increasingly, practices are no longer owned or run by physicians but by large groups, including hospitals. When looking at this graph, remember that not-for-profit is a tax designation, not a revenue statement – most major hospitals are not-for-profit only in the tax sense.
Increasingly, practices are no longer owned or run by physicians but by large groups, including hospitals. When looking at this graph, remember that not-for-profit is a tax designation, not a revenue statement – most major hospitals are not-for-profit only in the tax sense.
Shifting demographic desires
Another fundamental driver of this consolidation is the demographic shift in gender and age – older, male physicians are being replaced by younger and more female physicians. There are distinct differences in what we wanted or want from our careers. My generation had an assumed lifestyle that is no longer assumed – better in some ways, worse in others (at least to my mind), but not wrong, just different.
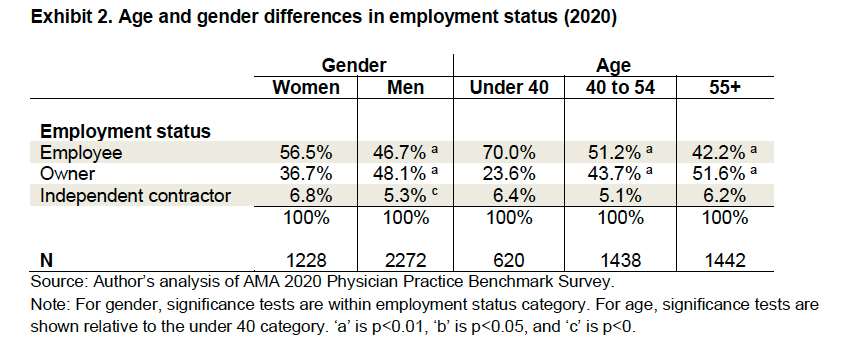 70% of the under-40 workforce are employees, not owners. [1] There are no billing headaches; there is a stable work schedule and vacations, far less uncertainty in the day-to-day business of medicine. I get it; it makes a great deal of sense. But there is a trade-off for that security; you are less autonomous, have efficiency goals to meet like patient throughput (patients seen per hour), social media likes, and patient satisfaction scores.
70% of the under-40 workforce are employees, not owners. [1] There are no billing headaches; there is a stable work schedule and vacations, far less uncertainty in the day-to-day business of medicine. I get it; it makes a great deal of sense. But there is a trade-off for that security; you are less autonomous, have efficiency goals to meet like patient throughput (patients seen per hour), social media likes, and patient satisfaction scores.
What’s in it for you, the patient?
Bigger can assure you of greater access, just not necessarily to “your” doctor. For physicians to have more of a work-life balance, you, as a patient, must be cared for by “any willing provider.” Pregnant women have been putting up with this for some time as they discover “their” obstetrician will not be there for the delivery; their partner, a willing provider, will fill in – after all, it is just a delivery. This type of “bait-and-switch” is found in many primary care and specialty practices and helps explain the increase in “concierge” practices where you pay more to see just one physician.
Specialization of physicians has advantages; there is a wealth of literature that more experience results in better outcomes. Care now requires a chain of physicians, each delivering their part of the finished product, your health. When you couple these care chains to the concept of any willing provider, your care is provided by a village. Unfortunately, when everyone is responsible, no one is responsible.
While it may take a village to provide sophisticated or complex care, to personalize care, you need just one. Having, let alone identifying, your doctor is the cost of changing practice patterns for the most vulnerable part of the healthcare system, the patients. [2] If your idea of personalized medicine is a test to see whether a genetic variant alters your treatment, then any willing provider can and will order the necessary testing. But if personalized medicine means insightful awareness of your needs and finding the right balance of observation, medication, and intervention, you are increasingly disadvantaged. Who is your special doctor in the chain? Where will they be if you need to make a decision more challenging than fixing a hernia or injecting your knee? As a physician, I find the real tragedy is that many patients, those under 50 or so with few medical issues, will never know what they lost, even after it is gone.
[1] This may include some physicians completing their training rather than physicians in practice.
[2] This particular care disparity is not necessarily due to race or income. Read a little about the care given to President Garfield or, better yet, the Shah of Iran, and you will see that being of a higher “caste” is no guarantee of better care.

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


