
1. Higher viral loads and longer transmission period
The study reported in medRxiv comes from China, where 167 cases of COVID-19 due to the Delta variant were identified from a single source [1] between May and mid-June of this year. All of the individuals (62) where the time of contact could be determined were followed with daily PCR testing. When compared to a control group of individuals diagnosed with the original COVID-19 variant, the tests became positive two days sooner. Viral loads were also significantly higher at the time of detection – 1260-times higher. These findings of increased viral loads were mirrored in nasopharyngeal swabs; the means we use to gather our samples and then use the PCR test to identify the presence of COVID-19. In those nasopharyngeal swabs, 80% were THE Delta variant, WHILE ONLY only 19% were for original COVID-19. Much of our modeling is based on the findings that it took about five days for the original COVID-19 (clade 19A/19B) to become infectious; the Delta variant requires only 3.7 days.
2. Breakthrough infections occur but are significantly less severe
The medRxiv study was conducted in Singapore, looking at patients who completed vaccination with an mRNA vaccine and subsequently developed a PCR-confirmed positive infection with the genomically identified Delta variant. They were compared with unvaccinated patients that were also PCR positive for the Delta variant. All patients in Singapore, symptomatic or not, are hospitalized. Those requiring supplemental oxygen were also treated with remdesivir; dexamethasone was reserved for those with progressive symptoms. Severe disease required oxygen; moderate disease only required chest X-ray evidence of a pneumonia. The study period ran from April to mid-June of this year. 32% of the 218 patients with the Delta variant had been fully vaccinated. (66% Pfizer). Only 9% of vaccinated patients were symptomatic, three-fold less (28%) than the unvaccinated. Biomarkers of severity were worse in the unvaccinated, as were the number of symptoms. Shortness of breath was seen in 13% of the unvaccinated, 1.4% in those having completed their vaccinations.
The study did not determine viral loads but used PCR replication cycles as their biomarker. As the graph 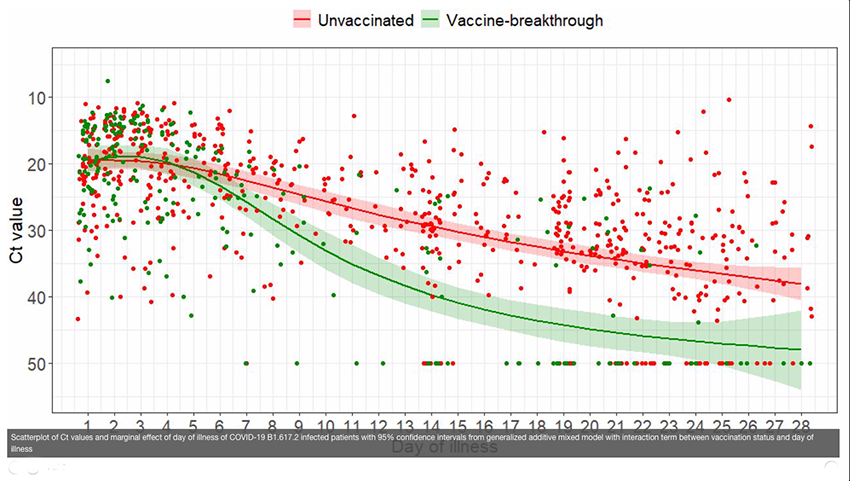 demonstrates, viral loads dropped more quickly in vaccinated individuals. More in-depth serologic analysis of a subset of both groups demonstrated a more robust immunologic response by the vaccinated. However, as you might expect, it was more directed at the spike protein configuration of the original COVID-19.
demonstrates, viral loads dropped more quickly in vaccinated individuals. More in-depth serologic analysis of a subset of both groups demonstrated a more robust immunologic response by the vaccinated. However, as you might expect, it was more directed at the spike protein configuration of the original COVID-19.
“Vaccine-breakthrough infections will continue to be observed, especially with genetic drift and selection pressures resulting in emergence of newer VOCs; however, it is likely that there will be a shift toward milder disease spectrum with more widespread implementation of vaccination programs.”
3. R0 is dynamic and changes over time
At the onset of the pandemic, R0, the infectivity of the original COVID-19 was calculated at five. With time it came down to around 2 or 3, slightly greater than seasonal flu or the norovirus. The innate infectivity of the virus is moderated by available hosts, in turn, impacted by population density. Vaccination is protective to a significant degree from the Delta variant; the unvaccinated have no protection. As we have more vaccinated individuals or survivors of a Delta infection, the number of available hosts will drop, as will the R0. The current comparison of the Delta variants infectivity to chickenpox will change over time.
What might we conclude?
Let’s assume for the moment that those two reports are in the right ballpark. They do not have to be exact. The Delta variant replicates more quickly and creating more infectious copies than the first iteration of COVID-19. As a result, asymptomatic individuals can spread larger viral loads to more people. Vaccination reduces disease severity for those infected and reduces their ability to transmit the disease to others. It does not eliminate transmissibility or your risk– that would be a miracle, not a medicine. Vaccination remains the key; it is the most protective option for ourselves and those around us. It works better than mask or lockdowns, but for reasons that many of us cannot fathom, the people who most vocally insist on not wearing masks and railing against lockdowns are not getting vaccinated. What up with that?
[1] Sources were identified through contact tracing or genomic analysis.
Sources: How the Delta variant achieves its ultrafast spread Nature
Viral infection and transmission in a large, well-traced outbreak caused by the SARS-CoV-2 Delta variant medRxiv DOI: 10.1101/2021.07.07.21260122
Virological and serological kinetics of SARS-CoV-2-Delta variant vaccine-breakthrough infections: a miulti-center cohort study medRxiv DOI: 10.1101/2021.07.28.21261295xiv

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


