What do you mean by a mask?
Quick review – the mask's purpose is to filter out microbial particles and prevent the transmission of the virus, in this case, from the mask wearer to others. To a lesser degree, it can filter out particles moving in the other direction from others to you, the mask wearer.
The filtration ability of masks varies with the material used. Simply put, homemade cloth masks do not work as well as paper “surgical” masks, which do not work as well as N95 masks. The fit of the mask also affects filtration; very few of us are wearing custom-fitted N95 masks, used mainly by medical personnel in "hot spots” or situations. Most of our health care workers are wearing off-the-shelf N95 or surgical masks; they are not custom-fitted.
To a large degree, fit and filtration ability are not as important as we might think. Most of the work about the transmission of COVID-19 involves respiratory droplets, a mixture of viral particles, water, and other expiratory secretions. These droplets are big enough that most masks effectively capture significant amounts of them, whether they are properly fitted or not. Masks are a physical barrier that impedes the transmission of COVID-19 – they are a speed bump on the transmission highway.
Scientific Studies
As my colleague Cameron English has pointed out, the scientific studies of the effectiveness of masks are all over the place.
Here are the findings of a study using influenza data to model outcomes.
“Our results suggest that the use of face masks at the population level can delay an influenza pandemic, decrease the infection attack rate, and may reduce transmission sufficiently to contain the pandemic. The effect on final size of the epidemic depends on features of virus transmission, mask efficiency, and coverage of mask use in the population.” None of the studies we reviewed established a conclusive relationship between mask/respirator use and protection against influenza infection."
And here is a meta-analysis of masks as a preventative measure.
“None of the studies we reviewed established a conclusive relationship between mask/respirator use and protection against influenza infection.”
We do not have quantitative, certain knowledge of the degree of protection afforded by non-pharmacologic interventions. I can cite or “cherry-pick” studies (verb choice depends on whether you agree or disagree with me) but cannot reach a definitive conclusion. We cannot “follow the science” because, at this moment in time, science is not showing us the way forward.
Real-world
The scientific method requires us first to formulate a hypothesis, e.g., masks work, and then design a study to test that belief. But we can learn without a theory based upon real-world observations. Humankind developed the six classical machines [1] without intellectual or quantitative information on how or what mechanical advantage is.
In that spirit, we have some very significant data on the use of non-pharmacologic interventions on influenza. They come from the NY State Department of Health that collects information on seasonal flu every year. Here is the graph that, for me, says it all—the number of patients hospitalized with laboratory-confirmed influenza.
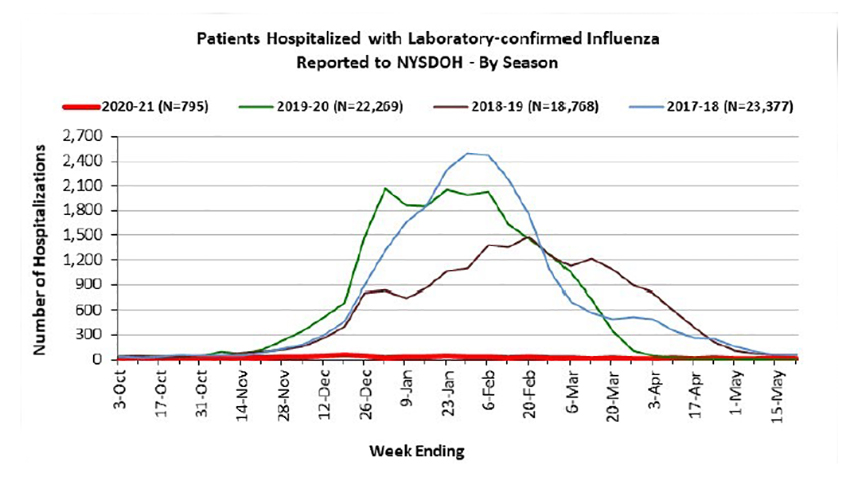 28-fold fewer patients were hospitalized for influenza in the last year than the previous year, 2,800% less! I would argue that it was our use of NPI that made the difference. When I mentioned this in our writer’s meeting, other concerns were raised that might explain this effect.
28-fold fewer patients were hospitalized for influenza in the last year than the previous year, 2,800% less! I would argue that it was our use of NPI that made the difference. When I mentioned this in our writer’s meeting, other concerns were raised that might explain this effect.
The 2019-2020 flu season did overlap a bit with the instructions to mask and social distance. That occurred in the latter part of February and extending into the rest of the year. The sharp-eyed amongst you will note that the decline in cases was somewhat greater than the previous year – an indirect suggestion of the efficacy of non-pharmacologic interventions.
Could it be more individuals being vaccinated? New York reports a 36% increase in influenza vaccinations; the CDC reports roughly an 11% increase nationally. Neither of these numbers seems to be sufficient to explain a 28-fold decrease.
Are seasonal flu and COVID-19 cross-reactive? By cross-reactive, I mean that they share surface structures that allow immunization from the seasonal flu to provide some partial immunity from COVID-19. Some preliminary studies show cross-reactivity, so the increase in seasonal flu vaccinations still cannot account for the large difference we see.
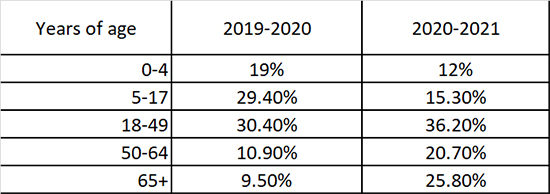 Could the influenza be different this year? The short answer is yes, at least when we consider confirmed infections by age groups. As an aside, the changes in children (age 0 to 17) shifted from 48% to 27% in one year, which should give us all pause in considering wearing the controversy over masks in school. The Delta variant seems to target different hosts than COVID original.
Could the influenza be different this year? The short answer is yes, at least when we consider confirmed infections by age groups. As an aside, the changes in children (age 0 to 17) shifted from 48% to 27% in one year, which should give us all pause in considering wearing the controversy over masks in school. The Delta variant seems to target different hosts than COVID original.
Could influenza have vanished? Perhaps the climate was so different that there was so little influenza to go around. But influenza and COVID-19 like similar environments. Let’s consider this magical thinking and move on.
Influenza is different from COVID-19. This is true in that COVID-19 is more infectious. Its R0 is higher, especially for the Delta variant, but as I have argued, R0 is dynamic, and it will come down and be closer to influenza over time. COVID is more clinically aggressive than influenza. From December 9th until March 6th, more people were hospitalized every day in New York than total hospitalizations for influenza for the 20-21 season. Part of that is because it is novel, and none of us have previously been exposed to this virus.
But seasonal flu and COVID-19 share one essential quality, they are both respiratory viruses that are transmitted through our breath. COVID-19 may shed more viral particles and for a more extended period before we become symptomatic, but those aerosolized particles are no different from those of influenza in size or shape. Our exposure to these viruses is most likely identical. No one is only capable of transmitting influenza or COVID. Our susceptibility, a necessary component of infectivity, does differ. We are more susceptible to COVID-19 because it is novel.
Seasonal flu is less likely to result in hospitalization because it has been around for a long time, and all of us have been exposed to one of its various forms. We have some degree of immunity. While we have little data on the protective effect of COVID-19 infections from reinfection, we do have increasing amounts of data on the impact of vaccination on “breakthrough” COVID. Vaccinations confer significant immunity; the vaccinated are anywhere from 5 to 161-fold less likely to be hospitalized with COVID-19 compared to unvaccinated individuals.
If masks and social distancing are so effective, why are there so many COVID-19 cases? Great question, and there is no good or bad answer. We have no previous experience for comparison. COVID-19 is novel, unlike influenza. We cannot draw valid comparisons using population data because we need to know the ages, co-morbidities, and exposures, and we simply do not have that information. If you believe that COVID-19 most resembles seasonal flu, then I think the changes wrought by wearing masks and social distancing on influenza are there for us to see.
Now, I am open to other scientifically plausible explanations. Still, I think we must conclude that in this last year, we heeded the annual advice of the CDC by covering our mouths and noses (with masks) when coughing and sneezing, wash our hands, and avoided exposing or being exposed to transmitters by social distancing. Those measures have greatly reduced infection by a respiratory virus. Without a good scientific reason why COVID-19 differs in how it is transmitted, we have real-world evidence that non-pharmacologic interventions work, in conjunction with vaccination, they work even better.
[1] “the wheel and axle, the lever, the inclined plane, the pulley, the screw, and the wedge, although the latter three are actually just extensions or combinations of the first three.” 6 Simple Machines: Making Work Easier
Sources: NY State Department of Health Weekly Influenza Surveillance Report

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


