
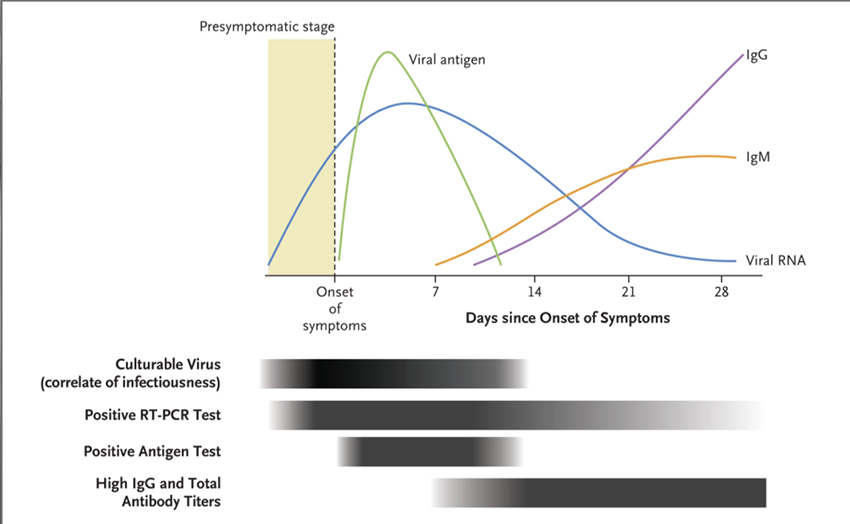
That one image captures what we know about the time course of the virus in our bodies, the onset of symptoms, and our immune response. Although not stated, transmissibility, giving the virus to another, is captured in a mixture of the viral RNA and antigen – it begins before we are symptomatic and diminishes but does not disappear in the 7-to-10-day period after symptoms develop.
The classic rapid diagnostic tests (RDT) for COVID are the RT-PCR test, which amplifies the viral RNA present, and antigen tests that look for “surface proteins, including the nucleocapsid, spike, and receptor binding domains, that are specific to SARS-CoV-2.” The at-home tests, the latest iteration of RDTs, are antigen tests. [1] Both tests have strengths and weaknesses, but, in general, antigen tests are more useful during the viruses’ transmission period – antigen tests identify the “Typhoid Marys” among us. PCRs identify all the victims, past and present.
PCR tests are more specific and sensitive than those antigen tests, but antigen tests do just as well during the period when an individual is most infectious to others – when the viral load is at its peak.
All the approved RDTs demonstrate an 80% “positive agreement” in the presence of the virus and a 98% “negative agreement” in its absence. But like all screening tests, their diagnostic performance – how often they can separate those with a disease from those without, varies with how likely the person being screened has the condition of concern, in this case, COVID.
My academic side would like me to spend the following few paragraphs talking about Reverend Bayes and his theorems, but you can find better explanations elsewhere. (Here is a wonderful video explanation.) Suffice to say; his sentinel work helped physicians understand how their opinions change based upon their initial feeling – Bayesian pretest and post-test probabilities. For our purposes, the NEJM article tells us how to interpret those RDTs based upon our belief that we are or are not infected with COVID.
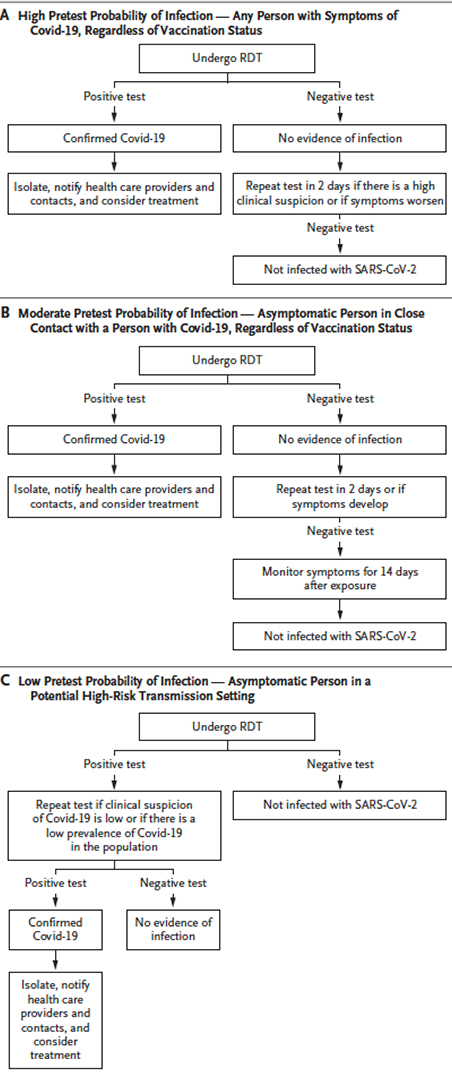 The accompanying chart provides the clearest guidelines for determining your need for a COVID RDT – be it PCR, lab-performed antigen, or self-performed antigen testing. It is based on our suspicion of having COVID before testing the pretest probability.
The accompanying chart provides the clearest guidelines for determining your need for a COVID RDT – be it PCR, lab-performed antigen, or self-performed antigen testing. It is based on our suspicion of having COVID before testing the pretest probability.
For those of us with symptoms [2], an RDT result is clear-cut when positive. When negative, it is worthwhile to repeat the test in two days if you remain symptomatic or your condition gets worse.
For those of us who had close contact with an individual diagnosed with COVID, most likely someone we live with or who has spent time in our homes, a positive test confirms the diagnosis of COVID. Out of an abundance of caution, and because it is difficult to know where we are in the virus's life cycle when we are asymptomatic, it is worth repeating the test in 2 days and being watchful for the onset of symptoms.
For the many of us, asymptomatic and without known contacts, crowding the lines for testing because a negative test is an entry requirement for school, work, or travel, a negative test means you are not infected. But because our pretest belief that you are infected is low, it means we should question a positive test result. It should be repeated, and only on the basis of the two positive tests do we diagnose an asymptomatic COVID infection.
[1] The term rapid is in relation to the time necessary for the “gold standard” of infectious disease diagnosis, a positive culture.
[2] The most common symptoms include fever or chills, congestion, cough, fatigue, nausea and vomiting, and of course, loss of taste or smell. Less frequent symptoms include a sore throat, headache, aches, pains, diarrhea, or rash.
Source: Rapid Diagnostic Testing for SARS-CoV-2 NEJM DOI: 10.1056/NEJMcp2117115

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


