
OK, first, let’s begin with the conflict of interest statement. I am a male surgeon, so my reading of the data may be biased. The study was published in JAMA Surgery, looking retrospectively at adults over age 18 undergoing various procedures in Canada between 2007 and 2019. The exposure variable was the concordance of gender between surgeon and patient, the outcomes, postoperative complications, re-admissions, and death. The data is from a single government payer, the Ontario Health Insurance Plan – the only requirement was being a resident of the province.
Here are the basics:
- 1.3 million patients, 2,937 surgeons, 600,000 gender concordant operations (83% male concordance), 717,000 gender discordant operations (male-female or female-male with 93% male surgeons)
- In the 30-day period after surgery 1.7% died, 6.7% were readmitted and 8.7% had significant complications
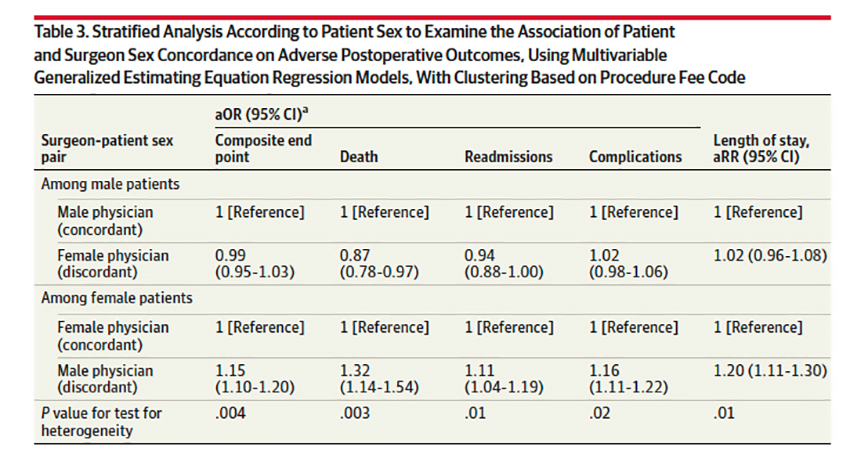 The table shows the results. A surgeon of either gender leads to the same outcomes for male patients. Having a male surgeon resulted in poorer outcomes for female patients, especially death. All of the findings are statistically significant, so I guess the case is closed. Good thing I hung up my mask, gloves, and knife.
The table shows the results. A surgeon of either gender leads to the same outcomes for male patients. Having a male surgeon resulted in poorer outcomes for female patients, especially death. All of the findings are statistically significant, so I guess the case is closed. Good thing I hung up my mask, gloves, and knife.
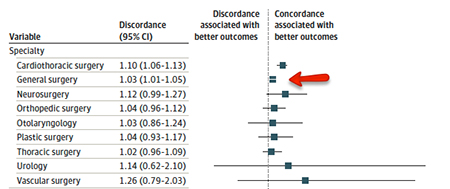 But before I fade away, there are a few caveats that might explain the findings beyond the simple idea that female surgeons are “better” in skills, judgment, or empathy – all determinants of outcome from a physician perspective. The first is that women have gone into surgery and its specialties at lower rates than men for many reasons. General surgery is the least skewed of the surgical specialties they considered, and when we look at discordant gender here, those percentages drop dramatically; the only place the discordant outcome holds is cardio-thoracic surgery [1]. In cardio-thoracic surgery, female surgeons performed roughly 8% of the total cases; for general surgery, they performed 20% of cases – so there is a question of a small sample size.
But before I fade away, there are a few caveats that might explain the findings beyond the simple idea that female surgeons are “better” in skills, judgment, or empathy – all determinants of outcome from a physician perspective. The first is that women have gone into surgery and its specialties at lower rates than men for many reasons. General surgery is the least skewed of the surgical specialties they considered, and when we look at discordant gender here, those percentages drop dramatically; the only place the discordant outcome holds is cardio-thoracic surgery [1]. In cardio-thoracic surgery, female surgeons performed roughly 8% of the total cases; for general surgery, they performed 20% of cases – so there is a question of a small sample size.
A more important distinction, one readily acknowledged by the researchers, is the role of comorbidities and severity of illness.
“…it is possible that, within each procedure examined, male surgeons may perform more complex or high-risk cases.”
The researchers suggest that there is no reason to anticipate more complicated cases for male surgeons, but in all instances, male surgeons were older and had higher case volumes – certainly consistent with the later entry of female surgeons into surgery and its specialties. They also noted that female surgeons treated younger patients with fewer comorbidities than male colleagues. The more experienced, more established surgeons have developed reputations and referral patterns that bring them the more demanding cases. That will change with time, and that will be an excellent time to repeat this study. Meanwhile, the lack of adjusting for patients’ “risk” makes for interesting reading but little instruction.
Gender discordance does have real impacts, especially for “situations of sensitive examinations.” There has been a rapid influx of female surgeons into gynecology and urology. Would you be more comfortable with a gender-concordant physician for those examinations? And as any married man can tell you, men do not “read” women, as women “read” one another, and that may well alter how symptoms and their severity are perceived. I am not sure any educational training other than experience corrects the disconnect in the genders fully understanding one another.
As is often the case, we are left with an enticing possibility and the need for
“Further sociologic research to evaluate how sex concordance, among other factors, influences patient-physician relationships, communication, and trust are warranted.”
[1] On a plot of this type, any value or confidence interval (the long horizontal line) that touches the vertical is insignificant. Only general and cardiothoracic surgery meet that criterion.
Source: Association of Surgeon-Patient Sex Concordance With Postoperative Outcomes JAMA Surgery DOI: 10.1001/jamasurg.2021.6339

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


