
“Prostate cancer is not only the most commonly diagnosed cancer among men, but it also carries with it one of the largest racial disparities in outcomes in oncology.”
Are these disparities biological or sociologic due to inequalities in social determinants of health (SODH) or some entanglement of the two? Some studies of large cancer registries report disparate outcomes between black and white men; some clinical studies have shown no effect. To find an answer, the researchers used a systematic review and meta-analysis.
Of 3832 possible articles, they winnowed the search to 47 studies in prostate cancer comparing the efficacy of care between black and white men with sufficient information to power statistical analysis. They categorized these 47 studies based on how many SDOHs were identified and “adjusted.” They accounted for the severity of illness, comorbidities, age, where they lived, income, insurance, and receiving standard care. [1] The most points were given for all the patients in a study having received standard care irrespective of insurance status. Studies could be high, moderate, or low in terms of the degree of adjustment made for SDOH.
- Type of treatment was documented in 96% of the studies, less than half reported clinical stage, and fewer reported standardized National Comprehensive Cancer Network risk stratification.
- Most studies considered age and extent of disease in adjusting for their regression analysis
- Few studies accounted for recognized disparities between black and white patients, including comorbidities, insurance, income, and geographic region. The mean number of adjusted variables was 2.
The researchers considered two outcomes. 53% of the studies reported prostate cancer-specific mortality, with a 76% overall survival. The combined studies demonstrated no significance in these outcomes between black and white patients. But a different picture emerged when the studies were broken out by their adjustment for SDOHs.
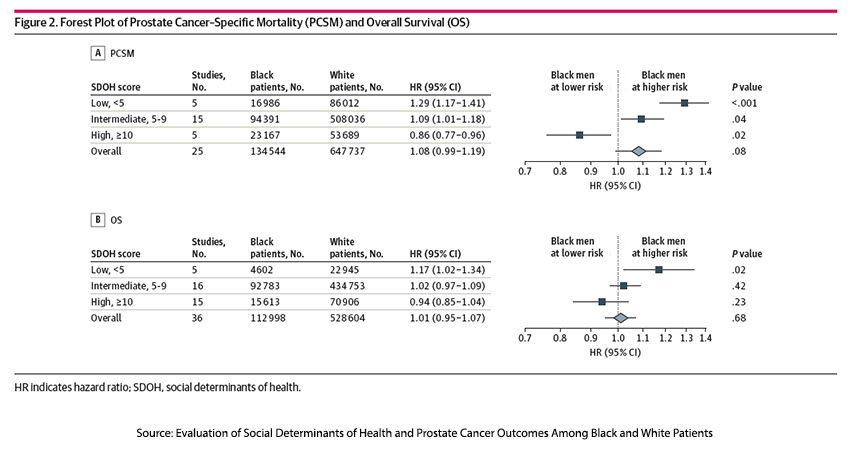
Studies with few adjustments for SDOH found that black men had poorer prostate-specific mortality and overall survival outcomes. When those additional social determinants were considered, the disparity in outcomes disappeared for overall survival and reversed, putting white men at more risk for prostate-specific mortality.
When Taken into account, SDOHs matter
The researchers note that the studies with a slight adjustment for these non-clinical factors would make it seem that prostate cancer in black males is somehow biologically more aggressive or lethal. But the disparities disappear when black men receive the same standardized care as white men and have equal access to that care.
“Encouragement of the biomedical community to transition from race-based to race-conscious research is critical.”
I would agree, as this study shows, that these social determinants may be missed when pursuing studies in which race has purely biological implications. I would prefer the term caste, which has specific social “inheritances” lost when thinking purely biologically. The researchers point out that communities of "persistent poverty (>20% of residents living in poverty for more than 40 years) had significantly higher cancer mortality rates,” irrespective of their racial makeup.
There are no quick solutions. Lack of access includes hesitancy on the part of patients to be screened and treated, not just a lack of insurance or a poor health network. There are limitations imposed by culture, education, employment, and even transportation. Many of these social determinants are not in healthcare’s “lane,” even though they may influence outcomes. Saddling the improvement in these determinants to health systems will ultimately mean, like other multitaskers, that they lose focus and provide suboptimal healthcare and SDOH mitigation.
[1] Here is the scoring system.
- Disease status: 3 point maximum - Diagnostic grade group or Gleason score (1 point) - Diagnostic PSA or PSA density (1 point) - Clinical or pathologic t-stage (1 point)
- Age: 1 point
- Comorbidities: 2 points.
- Insurance status: 2 points
- Income: 2 points
- Geography/Region of residency: 1 point
- Standardized treatment: 5 points
- Equitable/Harmonized Insurance benefits: 4 points
Source: Evaluation of Social Determinants of Health and Prostate Cancer Outcomes Among Black and White Patients A Systematic Review and Meta-analysis JAMA Network Open DOI: 10.1001/jamanetworkopen.2022.50416

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


