
The review involved 319 randomized controlled studies involving adults smoking tobacco at the time of entry, using one of the “approved pharmacotherapies and technologies used for smoking cessation worldwide [1] versus no intervention, a placebo, or another approved therapy. The outcome of interest was the number of individuals who had ceased smoking tobacco at six months and any serious adverse effects (SAE) of those therapies.
Using Cochrane’s well-accepted tools for assessing study bias [2]
- 51 of the studies were at low risk
- 104 at high risk
- 164 at unclear risk
- 118 reported pharmaceutical or e-cigarette/tobacco industry funding.
However, as the reviewers noted,
“Removing studies at high risk of bias did not change our interpretation of the results.”
Results
They found “high-certainty evidence” that e-cigarettes, varenicline (Chantix), and cytisine, a plant extract similar to nicotine that has been used for decades in Eastern Europe, all were “associated with higher quit rates than control.” Their use could increase the number of individuals not smoking by 8% - 8 out of 100 individuals, more than any of the control methods.
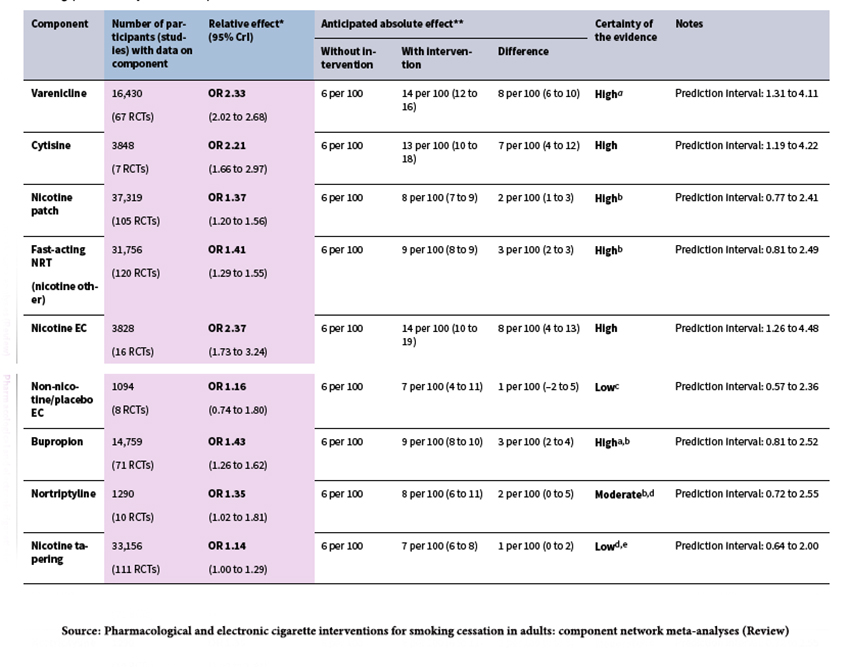 Nicotine EC refers to e-cigarettes utilizing nicotine and had the most significant effect overall – increasing those ceasing to smoke to 14, double that of the next most effective therapy, varenicline.
Nicotine EC refers to e-cigarettes utilizing nicotine and had the most significant effect overall – increasing those ceasing to smoke to 14, double that of the next most effective therapy, varenicline.
E-cigarettes act as a form of nicotine replacement therapy, and it is interesting to consider why they may be more effective than gum or patches. I would argue that smoking is both a physical and behavioral addiction. There is something about that first cigarette in the morning, over the first cup of coffee, or with co-workers that is more than physical dependence. It has a social aspect. Vaping allows for that sociability; it is hard to picture being asked to take a break while we all put on a nicotine patch or go outside to chew varenicline.
Serious adverse events were noted, greatest for bupropion followed by varenicline. The individuals impacted were far less than those helped. But we should be more concerned with long-term impacts which remain unknown and will develop over time. Specifically, we need to know more about the long-term impact of nicotine use as well as the possible effects of the non-nicotine elements involved in vaping (propylene glycol and glycerol).
E-cigarettes are banned in many countries. In the UK, New Zealand, and the EU, they are considered forms of nicotine replacement therapy. Our FDA, Canada, and Australia feel that they are tobacco products and not valid forms of nicotine replacement therapy. As a result, it is marketed as tobacco product, and its siren song of a "taboo pleasure" attracts teens.
Perfection remains the enemy of good
E-cigarette use should not be encouraged for the non-smoking public. But for the subset of people currently smoking, e-cigarettes, if we “follow the science,” may allow them to stop what we know is the most preventable cause of death and illness. There is no public appetite for banning tobacco in this country; otherwise, it would have already happened. And even if banned, our experience with Prohibition and now opioids tell us that prohibition would merely move tobacco use into the shadows.
Last word to the Cochrane reviewers,
“We are confident that e-cigarettes, cytisine, varenicline, nicotine replacement therapy and bupropion help people stop smoking. We do not expect more evidence will change these results. However, more evidence on how these treatments compare to one another, particularly in relation to harms, would be useful.”
[1] Those treatments include “varenicline, cytisine, nortriptyline, bupropion, nicotine replacement therapy (NRT) and e-cigarettes.”
[2] Bias in studies is judged to impact outcomes. They include selection, measurement, publication, and reporting biases.
Source: Pharmacological and electronic cigarette interventions for smoking cessation in adults: component network meta-analyses (Review) Cochrane Library

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


