
In a recent issue of JAMA, Dr. Anne R. Cappola, Director of the Penn Medical Communication Research Institute, takes a stab at providing strategies for better medical communication.
Episteme
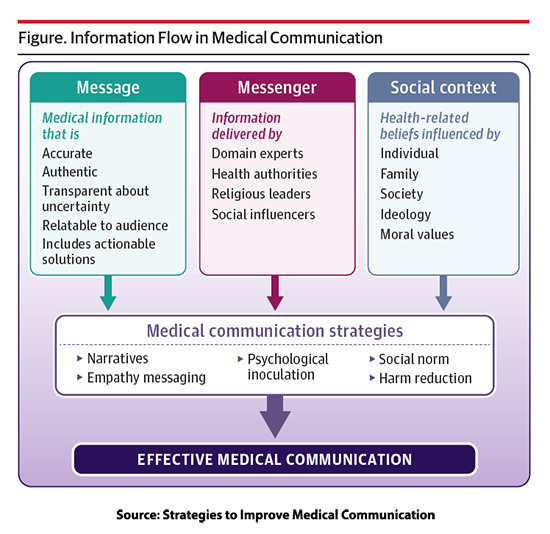
Dr. Cappola’s strategies are grounded in episteme – scientific knowledge and study.
“…clinicians can build trust by being accurate and authentic while communicating uncertainties about the evolving and sometimes contradictory nature of science.”
 What exactly is “being authentic?” I must confess that I turned to ChatGPT for an answer. “[Authenticity} involves aligning your outward behavior with your inner thoughts, feelings, and values, without pretense or external influence.” That seems a bit forced.
What exactly is “being authentic?” I must confess that I turned to ChatGPT for an answer. “[Authenticity} involves aligning your outward behavior with your inner thoughts, feelings, and values, without pretense or external influence.” That seems a bit forced.
“While information communicated (i.e., the message) should be based on evidence, narratives help connect the evidence to an individual.”
But nowhere in what Dr. Cappola wrote did she share stories to make those connections.
“Cultural and religious backgrounds influence health-related beliefs and how an individual responds to medical information. … People tend to favor information that reinforces their existing ideologies and identities and reject information that does not reinforce their preexisting beliefs—a process called biased assimilation.”
How many of us consider our thoughts and opinions “ideologies?” Just how can a physician or other individual reduce “biased assimilation?
“Harm reduction focuses on improving overall health by emphasizing reduction, as opposed to cessation, of risky behavior. By addressing the negative consequences of a behavior rather than the behavior itself, this strategy seeks to incrementally improve health and minimize adverse outcomes associated with a behavior.”
Nice theory, but to quote noted health communicator Yogi Berra,
“In theory, there is no difference between theory and practice. In practice, there is.”
Techne- skill and craft
This brings us to consider another term, techne or technical knowledge. It might also be called phronesis, practical knowledge or wisdom from countless patient interactions, not populations. Interactions where you can see the result of your effort more immediately, providing more useful feedback.
Almost no one comes to a surgeon’s office asking for an operation. If they do, you have to be suspicious. So much of the communication with my patients fits nicely within the framework of the basics of retail sales.
- Patient Focus - Understanding your patient’s health needs and treatment preferences is crucial. A good physician actively listens to identify patients’ needs and tailor the sales approach.
- Product Knowledge – you need a deep understanding of the treatment options. In the parlance of sales, this includes features and benefits. Medicine also requires knowing the risks and personalizing them as much as possible. In sales, unique selling points that differentiate your product from the competition are more overt; in medicine, you and your advice are the product, and your “bedside manner” often differentiates you from the surgeon or internist down the block.
- Building Relationships – building trust is critical. It is a product of their day-to-day experience interacting with you and your staff and, as I have written so often, more crucially, developing a long-term relationship.
- Effective Communication – clear and concise is crucial and often art rather than book knowledge. Physicians are most frequently problem solvers, so we need to meet our patients at their level of understanding. That does not mean acting paternalistically, but it does mean tailoring our message to meet their perceived needs.
- Closing the Sale – for some patients, their choice is clear, and closing is effortless. In other instances, there may be a hesitancy over the recommendation or you, the one making the recommendation. That is the time to be more like a fly fisherman, slowly reeling in the patient in their timeframe and concerns, not yours.
- Effective Merchandising – You are the product, so how your staff represents you and how you present yourself is critical. In the day, I had a ponytail, rebel that I was. But one quickly learns that everyone, at least in the Medicare age group I most frequently treated, wants the stereotypic surgeon “as seen on TV.”
Physicians of my and earlier generations thought of themselves as “professionals,” requiring a distancing from our patients and a formality of speech and dress. The paternalism of “we know best” did not require explanations, and the thought of “selling” a treatment was more akin to the purveyors of snake oil than the modern therapies we offered. The last 20 years of the corporatization of medicine have hopefully disabused physicians of their claim to being professionals and made it clear that they are labor – with a stethoscope substituting for a blue-collar. Academics and long-term bureaucrats are among the last bastions of physicians thinking of themselves as more than labor, and how they communicate health concerns harkens back to a much older time. The failure of messaging during COVID was partly due to medical leadership's inability to see themselves as retail salespeople.
Source: Strategies to Improve Medical Communication JAMA DOI: 10.1001/jama.2023.23430§

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


