
Let’s begin with a few generalizations:
- Black women have the highest prevalence of being overweight or obese
- Asian or Pacific Islander women have the highest prevalence of dense breasts
- The association between obesity and invasive breast cancer is stronger in postmenopausal women, and the association with breast density is stronger in the premenopausal.
Given these facts, it is clear that the women at risk for breast cancer will vary with the degree of obesity and breast density in the population at risk – breast cancer mammography screening cannot be a one-size-fits-all guideline. To dig a bit deeper into how the guidelines might be altered, the researchers looked at data from the Breast Cancer Surveillance Consortium (BCSC) containing data on self-reported race, menopausal status, age, mammographic findings, and any biopsy data.
To identify population attributable risk proportions (PARPS) [1], they used as their outcome identification of “advanced” cancer, more specifically a relatively small cancer, locally confined, with minimal if any lymph node involvement (Stage IIA). [2] The BCSC database yielded over 3. Million annual or biennial screening mammograms in slightly over 900,000 40- to 74-year-old women performed between 2005 and 2018.
- “Black women had the highest proportion of overweight/obesity (85.2%), followed by Hispanic/Latinx (70.4%) and White women (56.0%).
- Asian or Pacific Islander women had the highest proportion of dense breasts (65.4%), followed by White (46.6%), Hispanic (43.1%), and Black women(41%).
- Family history of breast cancer and history of breast biopsy was similar across racial and ethnic groups except for Asian or Pacific Islander women, who had the lowest proportion of both risk factors.”
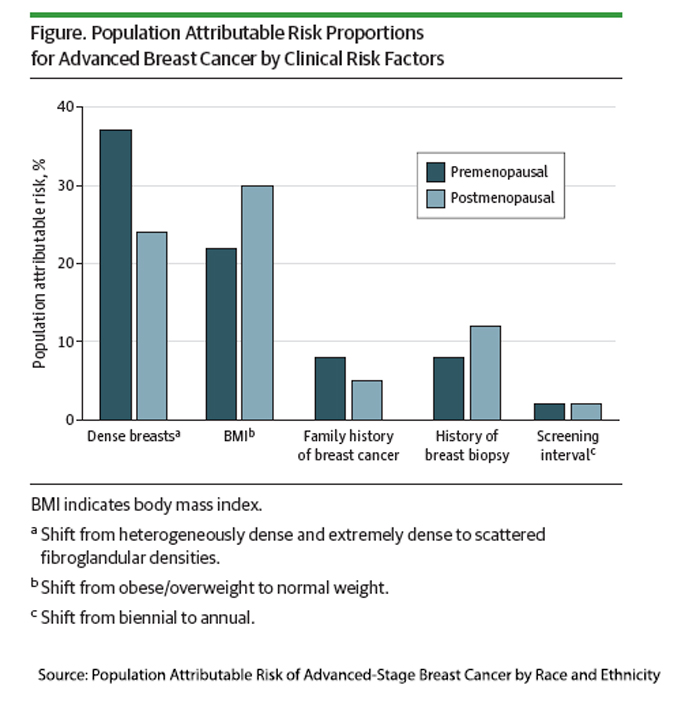
Quick note – These PARP percentages indicate how, if the risk factor was not present, the number of advanced cases of breast cancer was reduced.
- Screening frequency was a weak risk factor for advanced cancer, accounting for roughly 2% of attributable risk in either pre or postmenopausal women
- Family history accounted for a slightly greater proportion of advanced breast cancer diagnoses in this population, 8% in pre- and 5% in postmenopausal women. As the researchers noted, this runs somewhat counter to the general perception that a family history of breast cancer is the primary breast cancer risk factor.
- Being overweight or obese accounted for 30% of advanced cancer in postmenopausal women. The racial breakdown of these advanced cancers mirrored the racial incidence of obesity; Black women were far more at risk, with a 38% PARP than Hispanic women (31%) or White women (30%). The elevated risk for Hispanic women was a new finding contrary to prior research. It may reflect the outcome where obesity plays a greater role or a different subgroup of those self-categorized as Hispanic.
- Dense breasts accounted for 37% of advanced cancers in premenopausal women. Again, with PARP following the racial incidence – highest among premenopausal Asian or Pacific Islander (46.6) and White women (39.8).
There is little that can be done about breast density per se. Increased breast density reduces the sensitivity of mammography, increasing the false negatives, where cancer is present but not detected. It can also result in higher recall rates for additional, more sensitive screening, i.e., ultrasound or MRI. Current law in NY requires women to be notified that they have dense breast tissue and the risk of a false-negative. The FDA made this a national guideline in March 2023.
“Weight loss through diet and exercise and bariatric surgery in premenopausal and postmenopausal women have also been shown to reduce breast cancer risk.”
Will this become a new indication for GLP-1s? The impact of being overweight and obese is significant, resulting in anywhere from a 3 to 20-fold difference in advanced breast cancers. The researchers also note that weight loss may contribute to decreased breast density.
As with all studies, there are limitations. Most importantly
“Although reduction in breast density and BMI has been shown to reduce breast cancer risk overall, there is no direct evidence that reductions will lead to a decrease in advanced cancer risk.”
But it may allow us to fine-tune our mammography guidelines.
[1] Attributable Risk is the difference in the disease risk between individuals with and without a specific risk factor, indicating the additional risk the factor imposes. The Population Attributable Risk is the proportion of individuals in the population with that risk. The Population Attributable Risk Proportion (PARP) represents the proportion of disease cases in the entire population that could be prevented if the specific risk factor were eliminated.
[2] They used this stage as it has a highly predictable relationship to breast cancer mortality.
Source: Population Attributable Risk of Advanced-Stage Breast Cancer by Race and Ethnicity JAMA Oncology DOI: 10.1001/jamaoncol.2023.5242

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


