
While many of us have seen the ads for Attends, the problem being treated, urinary stress incontinence in women, is rarely mentioned [1]; and that is odd for a problem that by some reports effects 25% of women over age 25. (The incidence of breast cancer is about 12%). A recent article in the American Journal of Obstetrics and Gynecology sheds light on this somewhat unmentioned disease.
Urinary incontinence is the involuntary passing of urine, frequently associated with coughing, laughing or any activity that causes a person to bear down. It is a result of the loss of support for the bladder, rectum, and vagina – all the structures of the pelvis and is most often seen in women after childbirth. For all the beauty and miracles of birth, passing an eight-pound object through the vagina causes some wear and tear. But physicians know little about the natural history and progression of this loss of pelvic support (clinically termed prolapse). The study provides a better understanding of the course of the disease and some possible milestones.
The Study
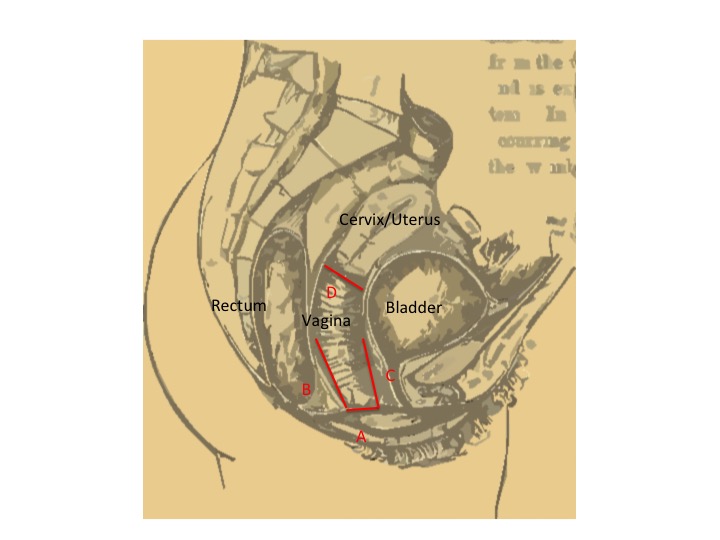 1224 women, five to ten years post the birth of their first child were followed longitudinally for up to 9 additional years. At the annual examinations, measurements were made of their pelvis, and they completed questionnaires of the symptoms associated with prolapse. The primary measures looked at the distances of the vaginal walls from the urethrae (C&D) – the opening through which we urinate – and the position of the cervix (B). They also measured the size of the opening of the vagina, termed the genital hiatus (A). Over the time of the study, 7,000 measurements were made. As pelvic support is lost, all of these distances, except for the genital hiatus shorten. The genital hiatus widens with declining pelvic support.
1224 women, five to ten years post the birth of their first child were followed longitudinally for up to 9 additional years. At the annual examinations, measurements were made of their pelvis, and they completed questionnaires of the symptoms associated with prolapse. The primary measures looked at the distances of the vaginal walls from the urethrae (C&D) – the opening through which we urinate – and the position of the cervix (B). They also measured the size of the opening of the vagina, termed the genital hiatus (A). Over the time of the study, 7,000 measurements were made. As pelvic support is lost, all of these distances, except for the genital hiatus shorten. The genital hiatus widens with declining pelvic support.
- 20% of women had no measurement changes, no evidence of lost pelvic support.
- Pelvic support was lost more rapidly in those women undergoing vaginal delivery rather than Cesarean section. [1] But women undergoing Cesarean sections also developed prolapse.
- The number of children a woman had delivered, their parity, did not influence the rate of change or loss of support.
- The change in the genital hiatus (A), the easiest to obtain measure, was a useful marker for loss of pelvic support overall.
- Most importantly, the loss of support was a gradual process over many years.
The reasons for the loss of pelvic support while related to giving birth are unknown. Mechanical trauma is an intuitive cause as the support structure of the pelvis are stress during delivery and may not fully recover. But there are other causes at play, including a hormone named relaxin, which among other actions softens the pelvic ligaments before birth presumably to allow the pelvis to expand. The underlying causes are at best ill-defined, but this study at least provides some information to the rate of progression, the time frame before patients become symptomatic.
The study provides a more dynamic understanding of disease progression, and it provides a clinically useful marker, the widening of the genital hiatus. When taken together they create an opportunity for physicians to intervene before the only recourse is surgery. Now perhaps we can begin to look more closely at the underlying factors and possible means of mitigation. For a disease affecting 25% of women and that results in 400,000 operations annually, that would be both a health benefit and healthcare savings.
[1] My colleagues have informed me that while urinary incontinence in women is not discussed in the media, it is a “hot topic in Mommy groups.”
[2] I and the authors hasten to state that this is not a reason to undergo a Cesarean section.
Source: Longitudinal study of quantitative changes in pelvic organ support among parous women American Journal of Obstetrics and Gynecology DOI: 10.1016/j.ajog2017.12.214

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


