By David Shlaes — Apr 15, 2019
If we're not likely to see a significant pull incentive in the United States (or anywhere else) this year, a likely outcome, where can we go next? There are two actions we can take that will help.

Months ago, long before the 2018 election, I was led to believe that Senate candidate Jackie Rosen of Nevada was seriously interested in working to solve the broken antibiotics market. In the months before the election and since then I have been speaking to the now Senator’s staff about this issue. I have sent them articles, documents, studies, and links to information on the internet. This week I learned that while the Senator is interested in learning about the problem, she is not ready to lead on the issue. She has not even seriously approached her colleagues in the Senate or the House on the subject. She is interested in making sure that the NIH has enough funding for antibiotic research. But as we all know, we can fund all the research we want, but without a market, it could be like flushing the money away.
My own congressional representative, Joe Courtney, has never said he would support pull incentives for antibiotic R&D. He is most interested in reducing drug prices.
I had planned on a visit to Washington, DC this week to speak to staffers on this issue. But I now realize that this would be a waste of my time and theirs.
In both these cases, reading between the lines, I feel that the prospect of providing financial support to the greedy pharmaceutical industry is anathematic. It seems like no one in Washington is willing to look beyond an upfront investment in such an incentive in order to realize future cost savings. This is like supporting prices for vaccines that have shown that they provide a ten-fold return on such an investment. We already accomplish that by reimbursing for many vaccines especially for children – see this National Academies Report. Many studies show that inappropriate antibiotic therapy given usually because of unsuspected resistance costs lives. Having the right antibiotics available to physicians and patients would clearly be a life-saving, and therefore, a cost-saving benefit. Why can’t we make this investment in our future and that of generations to come?
There is a new DISARM bill in the Senate. This bill would provide for reimbursement to hospitals for the use of expensive antibiotics active against resistant infection above and beyond the medicare diagnostic related grouping payment. While this is a step forward, its just a baby step. The problem is that it is reimbursement. Hospitals would still have to actually stock the new and expensive antibiotics in case they should see such a resistant infection, even if their usual incidence of such infections is low. That means they have to pay an upfront cost and may not be reimbursed if they do not use the drug. We also must remember that 70% of US hospitals are under 200 beds and 55% are under 100 beds. That is, most hospitals in the US are small community hospitals. They will be reluctant to take on these upfront costs. Most people I have spoken with only give this bill a 50/50 chance of passage – and its really a baby step.
If we are not likely to see a significant pull incentive in the US (or anywhere else) this year, a likely outcome, where can we go next? There are two actions we can take that will help.
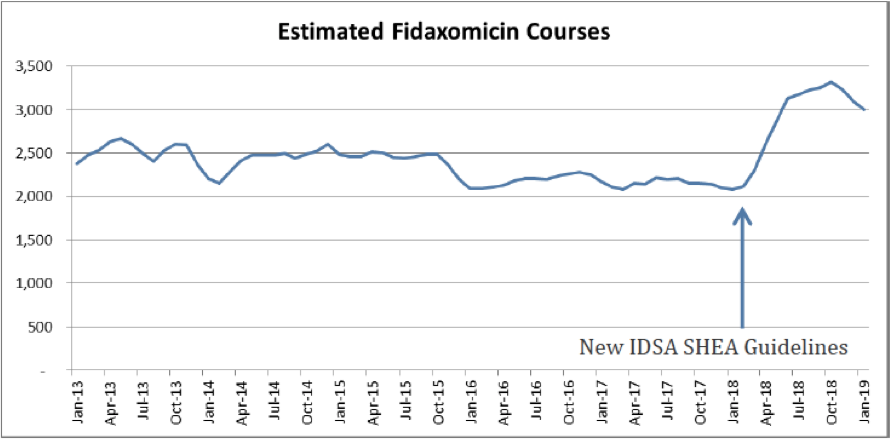
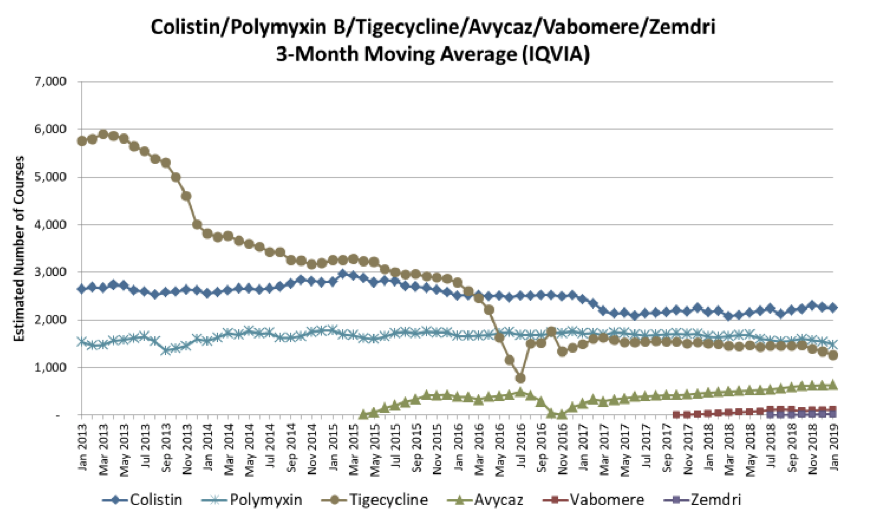
The first step is for the Infectious Diseases Society of America and perhaps the American Thoracic Society to provide clear clinical guidance that makes the use of colistin and polymyxin a practice of the past except in cases where there really is absolutely no other choice. The availability of new antibiotics like ceftazidime-avibactam, ceftolozane-tazobactam, meropenem-vaborbactam and plazomicin should all be prioritized over colistin/polymyxin for the treatment of Gram-negative infections where resistance is suspected or documented. Recent US data from Alan Carr on the use of Dificid for C. difficile diarrhea shows that guidance can make a huge difference in use (above). Compare that to the use of newer antibiotics for the treatment of carbapenem-resistant Gram-negative infections from the same report (below).
The second action item for us is to be sure that we can begin testing the susceptibility of pathogens to new antibiotics when the drugs come to market. Currently there is a one to several year delay that results in a delay in these new agents being used for treatment when they should be the drugs of first choice. This delay is mostly because of the way commercial susceptibility testing device companies run their business. This will be the subject of an entire blog in the near future.
If you were hoping for a significant pull incentive for antibiotic R&D this year, my advice is – don’t hold your breath. We need to turn our attention to insisting on new clinical guidance from the clinical organizations and thought leaders that relegates colisitin/polymyxin to the past. And we must hold the feet of the susceptibility testing device manufacturers to the fire and eliminate long delays between the launch of new antibiotics onto the marketplace and our ability to test pathogens to see if they are susceptible to treatment with these new agents. (This does not mean you should stop cajoling your representatives to pass pull incentive legislation).
###
Reprinted by permission of D. Shlaes. The original article can be found in his blog, Antibiotics - The Perfect Storm



