
Why do teaching hospitals feel the need to write articles justifying why they are better? What secret fear? Certainly not the rightfully discredited belief that the arrival of the new class of interns heralds a spike in hospital deaths. Don’t they believe that the “magic mirror,” US News and World Report showing the top 20 hospitals are all teaching hospitals? Well, for whatever reason, a new study looks at the value of surgical care provided at teaching versus nonteaching hospitals. [1]
A quick word on value, which combines two outcomes into a single number. Acting as the numerator is cost; the denominator, more often a clinical concern, mortality or readmissions. The value, in this case, the cost for a 1% improvement in mortality. For the study, researchers made use of CMS spending data for two years beginning in 2012, comparing general, vascular, and orthopedic surgical care of roughly 353,000 patients in teaching hospitals to “matched” patients receiving the same care in nonteaching or community hospitals.
Matching patients is a statistical idea where you pair individuals across a broad range of variables. “Matching ensures that comparisons… utilize pairs of patients undergoing the same procedure, who not only have comparable risk levels on admission, but have that risk for comparable reasons.” You can think of matching as a better form of multiple factor modeling, at least compared to standard regression analysis. But matched is similar, not the same.
The results
When comparing the two hospitals, for the teaching hospitals, mortality was lower and costs higher. Here is a summary. For those interested in “effect size,” the numbers are included and for the most part, are small. Of course, when it is you, any improvement in mortality is good.

Mortality considers all causes of death within 30-days of hospitalization, a standard measure. The use of resources is a modeling calculation of a hospital’s spending to provide care. There are several “costs” involved. There is the CMS payment for the initial hospitalization. CMS pays a fixed sum for operative care, so ICU use and length of stay lower hospital profitability. CMS payments also vary by geography, serving as a “disproportionate share” hospital [2], and indirect payments for training physicians. Finally, that cost number reflects the costs of physicians, the Emergency Department, and readmissions during that 30-day follow up.
The authors left two significant post-discharge costs out, the cost of visiting nurses or skilled nursing facilities, to my mind, definite limitations. After all, many of these patients receive that post-discharge care, it costs money, and the use of those services varies. The authors also calculated costs without increased payment by CMS for geographical site or training of physicians. I reported the costs without those variations, including them, increased CMS payments to hospitals. The bottom line, that cost to Medicare figure is a bit fuzzy, and perhaps a bit too low.
The value proposition is that teaching hospitals’ lower mortality is worth the additional cost – expressed as changing mortality/increased or excessive CMS payment. In aggregate, that 1% reduction in mortality cost $965 for a general surgery patient and $3546 for a patient undergoing vascular surgery; with a negligible difference in mortality for orthopedic patients teaching hospitals did not represent a more significant value proposition. The first thing that jumps out is the very low mortality associated with orthopedic care. Anyone working with orthopedists knows that no patient undergoes surgery without “clearance” by their primary care physician or cardiologist. Orthopedists prefer little, if any, risk, and while their surgery may be extensive, it impairs mobility more than vital function. For general and vascular surgeons, the risk is often higher and difficult to improve upon in the short timeframe necessary for treatment – you can’t spend a long time adjusting the lungs or heart in someone with a bowel obstruction or a dying foot. And those operations can impact or impair vital functions, like your blood supply or ability to eat.
A more interesting finding is when you look at how the mortality advantage of a teaching hospital changes with changing patient risk. Here is the study’s figure, the curve the increasing mortality advantage, the shaded area the 95% confidence intervals, and the box plot at the bottom, the number of patients. For those unfamiliar with box plots, they provide a way to visualize the distribution of patients. Most of the patients lie within the box, with the line to the left representing the lowest 5% of patients (5th percentile), the line to the right the 95th percentile.
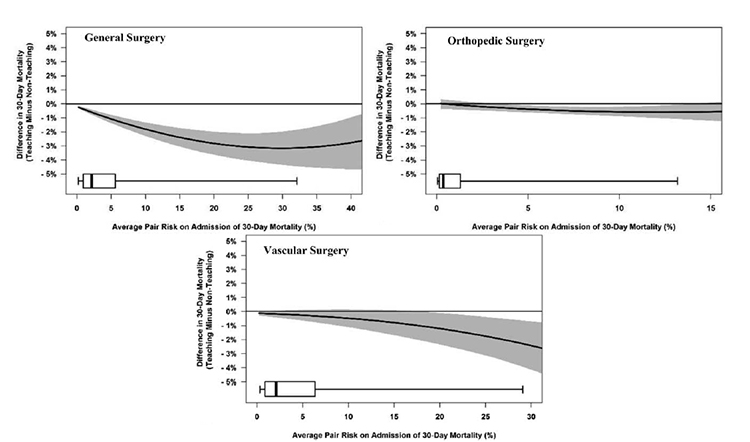
Look at orthopedic surgery, most of the patients are at low risk with little improvement in mortality. Vascular surgery has a larger box, a greater range of risk, but in that part of the mortality benefit curve, it is flat, with little change. For general surgery, that mortality benefit curve is steeper in the box where most of the patients are found. The takeaway, most patients will experience little mortality benefit obtaining their care at a teaching hospital over a community hospital. But patients at higher risk, a much smaller group, do achieve an advantage. So perhaps we should risk-stratify patients and refer patients at the highest risk to teaching hospitals and leave the rest in the community.
Of course, that would increase the cost of care at teaching hospitals because they would be spending more resources on the ill; and not get the cost savings and increased income from providing care to the relatively well. It would also enrich the experience of the trainees at the cost of additional experience for the community hospital, over time, lowering the ability of community hospitals to care for even those at a lower risk. As you already knew, it is complicated.
Teaching hospitals provide essential functions in caring for higher-risk patients and in providing adequate experience for physicians; after all, it is on the job training. Those two qualities alone make teaching hospitals worthwhile. Why they continue to feel they have to make a case for their cost, use of resources or value remains a puzzle. Perhaps it has to do with those accountants who would look at the expense of a 1% improvement in mortality?
[1] Many community hospitals have training programs in conjunction with a nearby medical school and its primary teaching hospital. They get the benefit of the halo of the medical school and a bump on their reimbursement from Medicare for providing physician training. The low ratio of the number of trainees or residents to hospital bed size separates these “pretenders” from the teaching hospitals being considered.
[2] Disproportionate share hospitals provide care to a disproportionate number of low-income individuals who pay nothing for their care.
Source: Comparing Outcomes and Costs of Surgical Patients Treated at Major Teaching and Nonteaching Hospitals Annals of Surgery DOI:10.1097/SLA.0000000000003602

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


