
Herd immunity seems to be a relatively simple idea. The fewer susceptible individuals in the herd, the more difficult it is for the disease to be transmitted. It is an equilibrium between infectious disease, be it a virus or bacteria, and its host – you know, a form of Darwinian co-evolution. The use of the term herd made me think that the concept arose from our study of nature, and while that is partially true, it had more to do with mice and measles than buffalos, cows, or sheep.
The first mention of "herd-immunity" is found in a paper from 1923 that chose to study the survivors rather than bacterial infection victims. In this instance, both survivors and victims were mice, and the researchers identified a problem that continues to challenge us, how the health of individuals translates to that of the community, the herd, and vice versa.
"There is definite evidence that, among a population containing susceptible and immunised individuals, the relative immunity of the latter does not save them from infection and death, when epidemic spread occurs. It appears that a degree of immunity, which may save individual hosts when living among equally resistant companions, is rendered of no avail when they are surrounded by highly susceptible individuals of their own species."
And in a practical way, they considered another problem we face again today, how to best distribute resistance.
"Assuming a given total quantity of resistance against a specific bacterial parasite to be available among a considerable population, in what way should that resistance be distributed among the individuals at risk, so as best to ensure against the epidemic spread of the disease, of which the parasite is the causal agent?"
 The resistance they described did not arise from natural exposure to a pathogen over the years, that Darwinian equipoise I had envisioned; it came from active immunization. A subsequent paper [1] looking at measles in children under age 15, living in Baltimore demonstrated some form of immunity within that herd. "Intact" in that study were individuals susceptible to measles. And you can see that herd growing larger after a measle's epidemic (case rates) and then dropping down to a persistent population. (For those believing there is little value in measles immunization, look at the frequency of those epidemics)
The resistance they described did not arise from natural exposure to a pathogen over the years, that Darwinian equipoise I had envisioned; it came from active immunization. A subsequent paper [1] looking at measles in children under age 15, living in Baltimore demonstrated some form of immunity within that herd. "Intact" in that study were individuals susceptible to measles. And you can see that herd growing larger after a measle's epidemic (case rates) and then dropping down to a persistent population. (For those believing there is little value in measles immunization, look at the frequency of those epidemics)
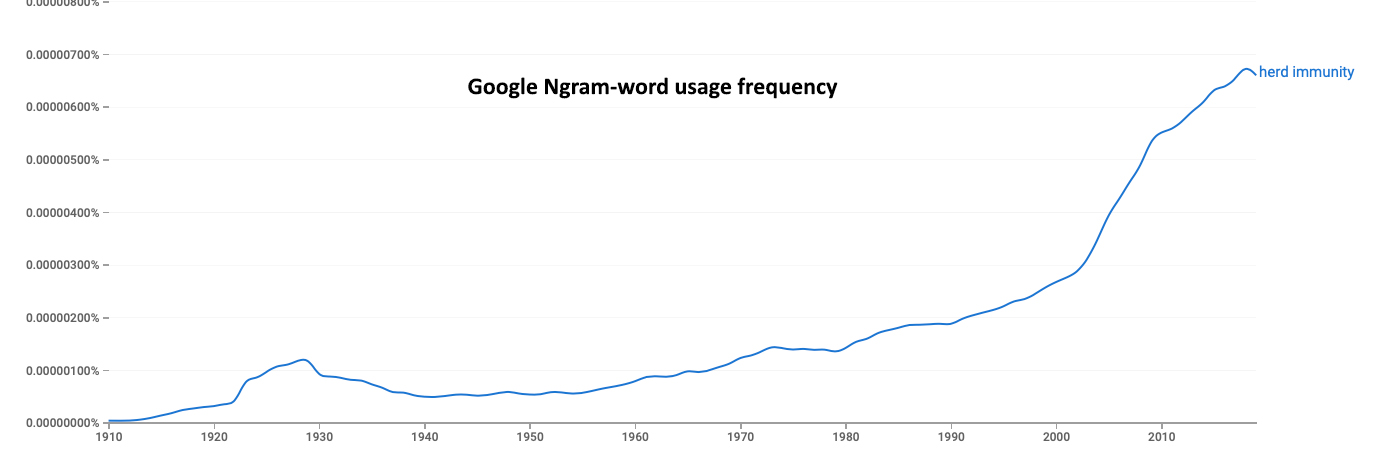 The term herd immunity remained linked to scholarly papers involving disease eradication, vaccinations, and their cost-benefit considerations until recently as the Google Ngram shows. Much of the study around herd immunity in the '70s later involved creating mathematical and computer models of optimum resistance patterns, provided by immunization, to mitigate disease. The initial models were threshold models, generating the numbers we hear in today's media, 80%, 60%, or 43%, the number of resistant individuals necessary to indirectly, through their immunity, protect others. But, "simple threshold theorem required random immunization and random exposure a degree of homogeneity that doesn't exist in reality." There were models and poor ones at that.
The term herd immunity remained linked to scholarly papers involving disease eradication, vaccinations, and their cost-benefit considerations until recently as the Google Ngram shows. Much of the study around herd immunity in the '70s later involved creating mathematical and computer models of optimum resistance patterns, provided by immunization, to mitigate disease. The initial models were threshold models, generating the numbers we hear in today's media, 80%, 60%, or 43%, the number of resistant individuals necessary to indirectly, through their immunity, protect others. But, "simple threshold theorem required random immunization and random exposure a degree of homogeneity that doesn't exist in reality." There were models and poor ones at that.
A review of herd immunity summed up the problem nicely,
"The magnitude of the indirect effect of vaccine-derived immunity is a function of the transmissibility of the infectious agent, the nature of the immunity induced by the vaccine, the pattern of mixing and infection transmission in populations, and the distribution of the vaccine—and, more importantly, of immunity—in the population. The nuances of immunity and the complexity of population heterogeneity make prediction difficult."
We know little about any of these salient factors for COVID-19.
We do know that imperfect, incomplete immunity, as well as waning immunity, requires increased levels and frequency of immunization. The 50% threshold for an effective vaccine, set by the FDA, is a good start, but it will not be one and done.
We know that the herd contains many different sub-herds, children, teens, high-risk, etc. We have little real understanding of how those group's varying susceptibility and immunity interact. Look at the difficulty of returning to school, where colleges seem to be different from elementary schools. There is no data to support or deny our fear that the children will transmit the disease to one another and subsequently share it with their teachers and families.
"Selective vaccination of schoolchildren against influenza was policy in Japan during the 1990s and was shown to have reduced morbidity and mortality among the elderly."
We know that transmission is more frequently within groups than across them. The recent epidemiologic data from India's track and trace bear this out for age groups. Most cases can be traced to households, rather than the public space.
Vaccination doesn't treat or cure COVID-19; it reduces transmission and indirectly protects us, like masks and social distancing. I've learned that herd immunity is neither a biological phenomenon nor an individual's immune response. It is a social phenomenon. Herd immunity is the result of our interactions. "One might argue that herd immunity, in the final analysis, is about protecting society itself."
While herd immunity theoretically can eradicate disease, in reality, "most programs aim at disease reduction to some "tolerable" level." The models suggest that vaccinating the superspreaders first is the theoretically optimum approach to quickly achieving herd immunity. But that requires them to be identified and high participation rates. It would also mean that high-risk individuals might be asked to wait, remaining quietly self-quarantined. By the numbers, many of our most significantly at-risk are ill-prepared for such social and financial sacrifice. And targeted vaccination will eventually result in "clusters of unvaccinated individuals," be they anti-vaxxers or those living within insular communities, no matter how carefully considered and planned.
[1] Monthly Estimates of the Child Population Susceptible to Measles, 1900–1931 American Journal of Epidemiology DOI: 10.1093/oxfordjournals.aje.a117929
Sources: The Spread Of Bacterial Infection. The Problem Of Herd-Immunity Epidemiology and Infection DOI:10.1017/S0022172400031478.
"Herd Immunity": A Rough Guide Clinical Infectious Disease DOI: 10.1093/cid/cir007

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


