
This one graphic makes a convincing argument that something is amiss here at home. Values greater than one indicate an increasing probability of dying compared to the 16 “control” nations. [2] Deaths of despair have been a growing problem for well over 50 years.
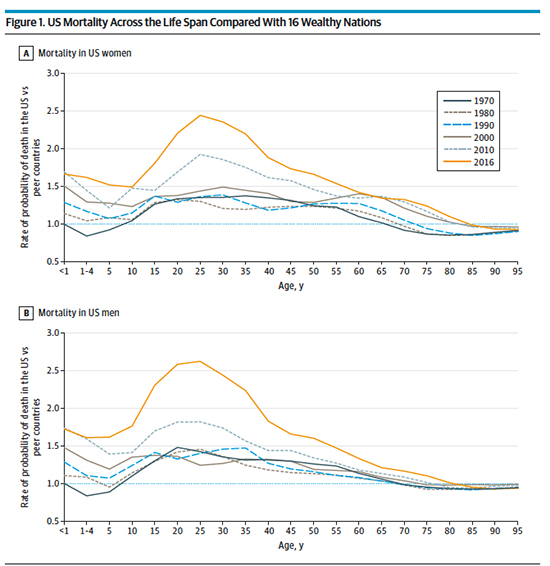
“…how do we understand right now why so many adults in the US, but not in the 16-nation control group,
lose the desire to live. What on earth is going on?”
The authors of this review critique a study done by the National Academy of Science (see sources). They begin by suggesting that biologically, we are all rewarded for seeking food, comforts, mates, and companionship – which seems a reasonable assumption. And that those rewards are hard-wired by dopamine that gives us a little boost and reinforces those experiences that aid in our survival. They suggest that our society and culture have reduced the episodic nature of those dopamine rewards, and like the clever monkey we are, we have found ways to potentiate its triggers. They write,
“…as modern life grows more predictable, the sources of surprise and their consequent dopamine pulses shrink. It is the difference between a day’s hard walk to finally encounter and kill a wild pig to feed the family and community vs. a quick trip to aisle 7 to select a pork roast in plastic wrap.”
In describing the drugs of substance use disorders, including alcohol and opiates, they point out that all of them remove the quick, transient dopamine pulse and replace it with a more sustained boost. It is not that the reward circuitry is diseased; we have altered its triggers to overcome its biological design. Again, the authors say it best.
“The body stores enough energy to allow fasting for days, but it cannot store satisfaction because that would silence the core circuit that propels us forward to meet the next need. By design, we are never more than a few small surprises from despair.”
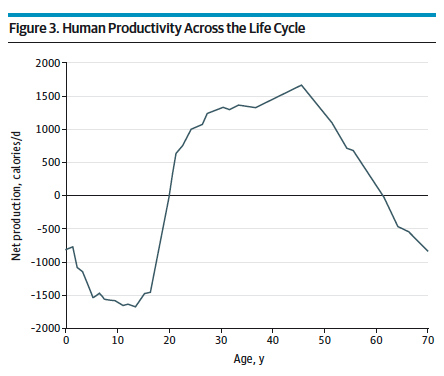 It is a well-accepted belief that we require a far longer childhood and adolescence than other animals, given our large brain size. A baby colt walks right away; a human infant typically requires a year. The figure to the left shows the calories hunter-gatherers (our biological ancestors) produced over their lifespans.
It is a well-accepted belief that we require a far longer childhood and adolescence than other animals, given our large brain size. A baby colt walks right away; a human infant typically requires a year. The figure to the left shows the calories hunter-gatherers (our biological ancestors) produced over their lifespans.
“…our species’ life cycle involves prolonged dependency with a significant transition at approximately 20 years of age to acquire adult skills. Historically, these were sufficiently complex to require 25 years of study and practice to reach maximum productivity, neatly coinciding with the final maturation of our frontal lobe.”
The authors suggest that much of our support system for those first 20 years has changed, citing alterations in family structure – from multigenerational to single parent. They believe that these changes make our period of dependency far more uncertain, with fewer dopamine-rewarded moments.
- Single-parent households have quadrupled over 50 years to 16 million, leaving 25% of all children in single-parent families.
- Single-parent households are 2.5 more likely to live in economic poverty, with 3-fold higher infant mortality.
- Increasingly, childcare becomes more fractionated or difficult to obtain
- Education, beyond high school, a key to financial success, is increasingly viewed as an individual responsibility – Student borrowing quadrupled between 2005 and 2015 with an average debt of $39,351. 6% of students owe more than $100,000.
The goal of the viewpoint was to point to differences between our statistics and that of those 16-control countries.
- Single-parent households are less common, with increases half that of the US.
- All provide prenatal and maternal care reducing premature and low birth weight infants “well below that in the US”
- They provide pre-school beginning at age three, and funding for education up through completion of high school is nationally funded, removing the disparities of funding that we see in our system. Six of the “controls” have no tuition college; 2 require less than $2,000. All have tuitions less than that of the US.
Many of those reading this will argue that this is the nanny state – cradle to grave economic support. What if we “flip the script” and consider the signal that is deaths of despair differently? What if, unintentionally, our social structure fosters defeat more than it supports success. What if it does take a village to raise a child?
“Every symptom of despair has been defined as a disorder or dysregulation within the individual. This incorrectly frames the problem, forcing individuals to grapple on their own—by learning resilience, self-help, and so on. It also emphasizes treatment by pharmacology, providing innumerable drugs for anxiety, depression, anger, psychosis, and obesity, plus new drugs to treat addictions to the old drugs. We cannot defeat despair solely with pills—to the contrary, pills will only deepen it.”
[1] “Deaths of despair”: The deadly epidemic that predated coronavirus Vox
[2] Australia, Austria, Canada, Denmark, Finland, France, Germany, Italy, Japan, Norway, Portugal, Spain, Sweden, Switzerland, The Netherlands, and the United Kingdom
Source: Why Deaths of Despair Are Increasing in the US and Not Other Industrial Nations—Insights From Neuroscience and Anthropology JAMA Psychiatry DOI: 10.1001/jamapsychiatry.2021.4209

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


