
Short answer – poor communication. Let’s take a deeper dive into a term we all know and hear but might not quite understand. What exactly is herd immunity, and how do we get it?
Herd immunity is
“when a sufficient proportion of the community in a defined area develops a threshold level of immunity to new infection that prevents exponential spread of infections in that community.”
The first words you should pay attention to are “our community” and “defined area.” Those terms help us to characterize the herd, which is not monolithic. The herd that is the US population consists of many smaller herds that can be stratified by their physical characteristics, like age or gender; by their location, in a particular state, rural or urban; and by their aversion (fear) of risk. That means there are many communities even within a defined geographic area. The herd of most significant importance consists of the people who surround you – your pandemic pod. Therefore, when we speak about herd immunity nationally, it is necessarily an aggregate of all those pandemic pods. A number, like 70%, is inherently uncertain, suggesting an aspirational rather than concrete goal.
“People were getting confused and thinking you’re never going to get the infections down until you reach this mystical level of herd immunity, whatever that number is. That’s why we stopped using herd immunity in the classic sense” Dr. Fauci
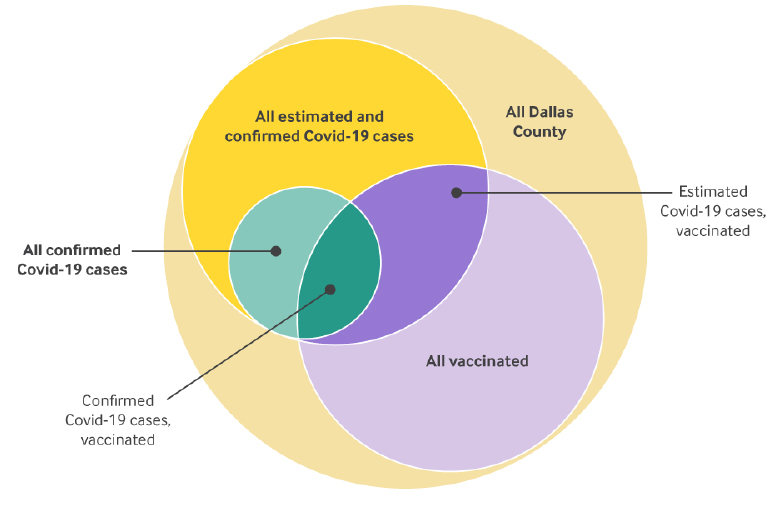
A new article in the New England Journal of Medicine’s Catalyst goes a long way in deciphering the rest of herd immunity’s definition. It is based on the SIR model. To refresh your memory, the acronym stands for Susceptible, Infected, and Recovered. We achieve herd immunity when there is no longer exponential spread of infection
“Herd immunity is dynamic and depends on the transmissibility of each new Covid-19 strain, the effectiveness of previous immunity due to previous infection and vaccination against these strains, and human behavior in local communities.”
Exponential spread requires susceptible individuals and transmittable disease. If we hold transmission constant, we can see that the more susceptible among us, the greater the spread. That was the case early in the pandemic, as COVID-19 original rampaged through the institutionalized frail and the highly exposed essential workers. If we hold the number of susceptible constant, increasing transmissibility will increase the spread. That is the case with the Delta variant that is far more contagious than its older siblings.
We cannot control the mutation of COVID-19 directly; that is our hubris. As Dr. Osterholm suggested, "We've ascribed far too much human authority over the [COVID-19] virus."
How can we reduce the susceptibility?
Several components make up our susceptibility that are fixed and cannot be altered. Our age, gender, and co-morbidities come to mind. The strongest of the two tools we have is our immune system; the other, controlling our exposure.
Our immune system, once exposed to COVID-19, in most cases leaps to our defense. Infection-acquired immunity works but comes at a price. As of this week, the CDC reports a total of 44.5 million cases of COVID-19, with a mortality of 1.6% and an incidence of severe adverse effects of 1%. [1] Vaccine-acquired immunity works well too, 188 million Americans have been fully vaccinated, with mortality of 0.0021% and an incidence of severe adverse effects of 0.000015% [2] Vaccine acquired immunity is far safer.
The current data suggest that infection-acquired immunity is more robust than vaccine-acquired when considering reinfection or breakthrough cases. We have no good numbers on reinfections among those with infection-acquired immunity, but for the sake of argument, let's put the number at zero. The CDC reports 6,617 deaths and 16,889 hospitalizations for breakthrough infections after vaccination. That would move the total mortality from vaccination to 0.0022% and severe adverse effects to 0.000104%. Vaccination remains the safest alternative, end of discussion.
But I have digressed. The critical feature when discussing herd immunity is that both infection and vaccine acquired immunity make you less susceptible. By my calculation, we have reached 70%. The second tool in our armamentarium is controlling exposure. We can control many of our direct contacts when we stick with our pandemic pods. Of course, that means we have to rely on our pod partners to be equally vigilant. Alternatively, we control our exposure by the use of masks and social distancing – “the human behavior in local communities.”
The entanglement
We’ve identified three different relationships between susceptibility, immunity, and our behavior. These relationships are not linear; they do not combine in easily charted straight-line relationships. And there are other relationships. For example, the greater the number of susceptible, the greater the reproduction of the virus, and given even a small but consistent rate of mutation, the greater the rise in variants. Not all variants are fit, in a “survival of the fittest” sense, but there will be the occasional one that is – call it Delta. Infectivity, Delta’s unique fitness quality, can also be diminished not just by reducing the number of possible hosts but in the ability of the virus to get fitter. The protection conferred by immunity wanes with time; we see it with both infection and vaccine-acquired immunity, so the time of vaccination in a population and whether or not they augmented that waning protection with a booster also will change.
Finally, of course, our behavior is subject to change too. Some remain hyper-vigilant. I am sure you have seen those masked and gloved, shopping for groceries. Others dutifully wear a mask in situations where they may be in direct contact with individuals where you have no idea of their level of infectivity (now a measure of the asymptomatic transmitters and the immunized). Others righteously declare their independence from the rest of the herd. And still, others try to do “the right thing” and manage to do so, some of the time.
All of these inter-related variables and their changing relationships result in cases, hospitalizations and deaths. That is why there is no specific number in achieving herd immunity. It is a dynamic dance between our species and COVID-19. We deploy our weapons and defense, as does the virus. There will be an equilibrium, and that will be the number we say in hindsight represents herd immunity.
[1] I am defining severe adverse effects as hospitalizations as reported by the CDC for laboratory-confirmed cases. The percentage of severe adverse effects may be higher if we count hospitalizations without laboratory confirmation but with high clinical suspicion.
[2] Using VAERS reported cases of thrombosis (29), Guillian-Barre (228), myocarditis (1640), and anaphylaxis (940)
Source: Rethinking Herd Immunity: Managing the Covid-19 Pandemic in a Dynamic Biological and Behavioral Environment NEJM Catalyst DOI: 10.1056/CAT.21.0288

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


