
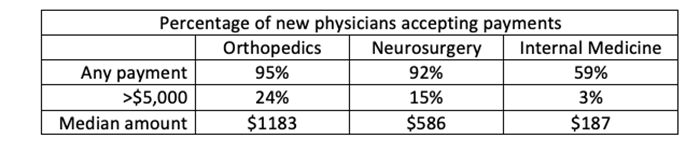
The study reported in JAMA Network Open looks at data from the Open Payment Database (OPD), which requires pharmaceutical companies and medical device managers to list their payments to physicians annually. That data was correlated with information on the physicians gender and dates of completion of their fellowship or residency training, so the researchers only considered payments to physicians during the first six years after their training.
They considered two surgical specialties, orthopedics, and neurosurgery, and used a medical specialty, internal medicine, as their “control.” [1] Let me use this table to summarize their findings:
Let’s begin to break down a bit of what was not said. The study considered what the OPD calls “general payments.” This includes fifteen categories, but I will restrict the unstated data to the top few, food and beverages – the free lunch, speaking fees, consulting fees, and royalties and licenses.
Skew U
When talking about averages, the underlying assumption is that the distribution of values, its range, is symmetric – the “bell-shaped” curve. There are three values you might employ,
- Mean – what we think of as the average
- Median – the number in the middle of the range
- Mode – the most common number
But this is not always the case, and the relative asymmetry from the bell shape distribution is described as the skew of the distribution. As the skew increases, the mean, median, and mode become very different, which is the first problem with the values expressed in this study.
The following examples come from the Open Payments 2019 dataset, a subset of the data used in the study. I would suspect that while the numbers might change slightly, the relationships and relative amounts are stable over time. For transparency, you can find the dataset and my calculations here. (Click download in upper left corner to view spreadsheet)

Dramatic differences
There is another problem with a skewed distribution, outliers – values that lie far away from most of the others and distort the average, median, and mode.
While we can all agree that payments for royalties and licenses to physicians are indeed a financial arrangement, it is hard to argue that these monies influence prescribing behavior. After all, if the physician invented the device, they already are using it. Royalty and licensing fees dramatically skew the amounts to the right, contributing 46% of all orthopedic payments, nearly 80% of all neurosurgical payments, and for internal medicine, a negligible 1%. How might average, median, and mode look if we removed those numbers?

There is little change in the Internal Medicine numbers, but a dramatic change in the average payments for both neurosurgery and orthopedics. The choice of what categories to aggregate and what number to use to describe that aggregation (distribution) matter.
Finally, if we look deeper into those general payments, the most common category is food and beverage. Considering these payments alone, what do we find

Most of these new physicians, two-thirds of orthopedists, 80% of neurosurgeons, and 91% of internists are getting less than $50 in free food – not quite the dire payola scandal and corruption of physician integrity suggested by the researchers.
The narrative – let’s get real.
“… small gifts from industry to physicians may seem to be inconsequential. However, research suggests that small gifts, even a single meal valued at less than $20, can be associated with unconscious bias in physician decision-making (e.g., in medication prescription). Thus, we considered that a physician accepting the first industry payment of any amount as developing a financial relationship with industry that can potentially influence physician behavior.”
The two groups they chose, orthopedists and neurosurgeons are device-driven specialties; there are few medication options that these surgical specialties pursue. Devices, on the other hand, are a different story. But ask yourself, in the real world, what control do these newly minted specialists have over the devices they use? Short answer, very little.
Most physicians recently completing their training are most comfortable using the devices they trained with. When they work in a new setting, they rarely decide what devices to use. Most of their senior partners have made choices, and their practice or hospital is a “Medtronic” or “Boston Scientific” shop. More importantly, those decisions by senior physicians are always in conjunction with the hospital, which tries to limit device choices so that their buying cooperatives will give them the lowest prices. [3]
All those free meals, and all those budding financial relationships; for the most part, reflect the presence of sales personnel in operating rooms. Sales personnel are not there to guide the surgeons; they are there because they bring the range of inventory they might need and the instrumentation required to implant their devices. Like any good guest, they do not come with empty arms; they bring lunch for the staff in the rooms.
Now because of the open payment rules, at least one physician will be asked to sign that the meal was provided. Resident and fellow signatures do not count, only attending physicians do. So the reality is that residents and fellows have been getting free lunches throughout their careers. Their initial prescription habits are more dictated by their training than by some independent thought. And as for speaking fees, like the previously mentioned royalties, you are not asked to speak as an inducement for your use of a device; you are asked to speak to induce others.
As I write this, a new target for the conflict-of-interest watchers has arisen, advanced clinical practitioners (nurse practitioners, physician assistants, CRNA, etc.). According to a recent JAMA study, they, too, are “on the take.”
[1] Orthopedics includes several subspecialties, sports medicine, spine surgery, adult reconstructive surgery, hand surgery, trauma surgery, pediatric orthopedic surgery, and foot and ankle surgery. Similarly, internal medicine includes several subspecialties, including critical care medicine or pulmonary medicine, cardiac or cardiovascular disease, oncology or hematology, gastroenterology, nephrology, rheumatology, endocrinology, and infectious diseases.
[2] One more point, orthopedists are receiving an average of $108,298 for speaking, which clearly is an outlier. A deeper dive into the data shows that just five events out of 641 speaking engagements explain 94% of that spending; I suspect an error in the submitted data.
[3] The cost of devices is not necessarily paid separately from the procedure itself. For example, nearly 50% of the payment hospitals receive for the endovascular repair of an aortic aneurysm goes to pay for the implanted device.
Source: Trends in Industry Payments to Physicians in the First 6 Years After Graduate Medical Training JAMA Network Open DOI: 10.1001/jamanetworkopen.2022.37574

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


