
I can’t believe we’re having this discussion in September 2023, just as the fall respiratory virus season commences and we're experiencing a new wave of COVID-19, but the politicizers of COVID won’t let up. Consider the ill-timed article by John Tierney in City Journal on August 27th claiming that “maskaholics are incorrigible” and everyone should reject masks because “we’re rational”.
Unfortunately, the SARS-CoV-2 virus, which causes COVID-19, is not rational. It mutates randomly, and then is subject to the rules of Darwinian evolution; the fittest progeny survive and proliferate. A variant called EG.5 (dubbed “Eris”) is currently dominant, but two new ones, BA.2.86 (“Pirola”) and FL.1.5.1 (“Fornax”), have emerged. Laboratory studies of BA.2.86 have found that it is able to escape our neutralizing antibodies 2-3 times better than XBB, the most recent Omicron subvariant to sweep the U.S.
Together, they are driving yet another surge. COVID hospitalizations and deaths have recently increased about 20% week over week, wastewater concentrations of virus are trending up, and there has been a report of a superspreader event in Nashville, and a probable one at the U.S. Open Tennis Tournament in New York after the organizers foolishly dismantled all precautionary measures. Various schools, hospitals, clinics, and other institutions around the U.S. are again requiring people to wear masks.
Tierney, a contributing editor at City Journal, has long been on a tear denouncing masks. Last February, in his piece “Approximately Zero,” he tried to make the case that “masks make no difference in reducing the spread of COVID — a claim I debunked shortly after. Now, with cases unmistakably trending upward, he’s back misrepresenting various studies and cherry-picking others.
Tierney again spins the meta-analysis by the Cochrane Library, a highly-respected British nonprofit that specializes in systematic reviews of health care interventions. Released last January, it has been fuel for the fire for mask skeptics. A top line reading of Cochrane’s conclusion might appear to support Tierney’s rants. As did many mask rejectionists, he quoted its conclusory statement that wearing a mask in the community “probably makes little or no difference” in reducing the spread of COVID, or any respiratory disease for that matter.
“The pooled results of [randomized control trials] did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks,” the review reads.
Tierney appears to have stopped reading the report after that headline, however, because the details paint a more nuanced picture that undermines his mask-rejectionist thesis. In fact, the researchers didn’t even study what Tierney mistakenly thinks they did.
Cochrane didn’t study the effectiveness of masks during COVID. Rather, they reviewed 78 studies, only six of which involved the COVID pandemic and only two of which specifically studied COVID and mask mandates. (And those two focused only on with whether mask mandates were in place but not the actual wearing of masks.)
The data in those few cases were so fragmentary and noisy, the Cochrane researchers concluded, it was impossible to draw any firm conclusion:
The high risk of bias in the trials, variation in outcome measurement, and relatively low adherence with the interventions during the studies hampers drawing firm conclusions. …
There is uncertainty about the effects of face masks. The low to moderate certainty of evidence means our confidence in the effect estimate is limited, and that the true effect may be different from the observed estimate of the effect.
Died-in-the-wool mask rejectionists jumped on the ambiguities, selectively twisting the findings. Fox News led the charge:

The confusion spiraled when the lead author of the report, Tom Jefferson, an Oxford University tutor, told conservative columnist Bret Stephens of the New York Times, “There is just no evidence that they” — referring to masks — “make any difference.”
It’s perhaps understandable that there was some confusion in the days after the release of the muddy-worded Cochrane report. But soon after. the Library’s editor-in-chief, Dr. Karla Soares-Weiser, weighed in, rebuking Jefferson for extrapolating on the very thin data. “That statement is not an accurate representation of what the review found,” she told the Times. Soares-Weiser then released a statement posted on the Cochrane’s website:
Many commentators have claimed that a recently updated Cochrane review shows that ‘masks don’t work’, which is an inaccurate and misleading interpretation. Given the limitations in the primary evidence, the review is not able to address the question of whether mask wearing itself reduces people’s risk of contracting or spreading respiratory viruses.
Thousands of studies underscore the consensus that masks do limit infections and spread. A meta-review published last month by British and Canadian scientists used 5185 unique records of studies performed from the start of the pandemic to January in asking whether: (i) wearing a face mask; (ii) wearing one type of mask over another, and (iii) mandatory mask policies can reduce the transmission of SARS-CoV-2 infection, either in community-based or healthcare settings. Their conclusion:
More studies found that masks (83%) and mask mandates (89%) reduced infection than found no effect (12%) … Despite the [risk of bias], and allowing for uncertain and variable efficacy, we conclude that wearing masks, wearing higher quality masks (respirators), and mask mandates generally reduced SARS-CoV-2 transmission in these study populations.
Children, schools and mask mandates
But Tierney and his ilk are having none of this. Now they are criticizing mask mandates for endangering the health of children. He cites “an extensive analysis” published earlier this year which found that a mandate had no significant effect on cumulative COVID infections or mortality, but did correlate with one statistically significant effect: a decline in fourth-graders’ test scores. He characterizes this as “an example of the singular cruelty of America toward children.”
Contrary to Tierney’s (mis)take, here are the relevant conclusions of the study:
State governments’ uses of protective mandates were associated with lower infection rates, as were mask use, lower mobility, and higher vaccination rate, while vaccination rates were associated with lower death rates. State GDP and student reading test scores were not associated with state COVID-19 policy responses, infection rates, or death rates. [emphasis added]
Tierney also goes off in a tirade against what he says is the “possibly toxic effect of prolonged mask-wearing, particularly for pregnant women, children, and adolescents” — the now familiar and notorious “killer mask” claim. His new evidence? A review article published last March by a team of German researchers which concluded a “need exists to reconsider mask mandates … due to chronic carbon dioxide re-breathing.” Another City Journal columnist hyped it in a May column, “The Harm Caused by Masks.”
This “new, but old” killer mask claim has been a conspiracy theory trope since the beginning of the pandemic. In this latest iteration, the German authors, none of whom is an expert in this field and include a veterinarian and a psychologist, posit a made-up malady, “Mask-Induced Exhaustion Syndrome (MIES).” But even they acknowledge there are not much data to support their grandiose warnings: “Overall, the exact frequency of the described symptom constellation MIES in the mask-using populace remains unclear and cannot be estimated due to insufficient data.”
The myth took wings in 2000 when graphics like this circulated on social media.
Then a video meme of a woman breathing directly onto a carbon dioxide monitor while wearing a COVID-19 mask was posted, and blew up Facebook. She claimed to have a “professional carbon dioxide detector” which would beep when CO2 levels reach dangerous levels. Within seconds, the reading skies from 1,895 to 10,000 while the device beeps furiously. “This is dangerous,” the woman says solemnly.
Not true. “You can repeat this experiment without a mask and you will get the same result,” Lidia Morawska, the Director of the International Laboratory for Air Quality and Health at Queensland University of Technology, told Reuters.
Why? The test is bogus for the same reason the claims in the German study don’t make scientific sense. As the U.S. Centers for Disease Control and Prevention (CDC) explains, carbon dioxide could not possibly get trapped in a mask.

Dr. Victoria Forster, a cancer research scientist, elaborates in Forbes:
Take surgeons, for example — during long procedures, they wear surgical masks for hours with no ill-effects on their carbon dioxide levels. Having a surgeon with an altered mental state would not be in the best interests of either the patient or the surgeon and thankfully, this simply does not happen…
What about tighter-fitting masks made from denser materials, such as N95 masks, worn by some healthcare workers coming into close contact with COVID-19 patients? Well these, only if fitted appropriately, will filter out coronavirus particles. But they do not protect the wearer from gases and small molecules which freely pass through the filter as they are just too small.
Although there is a reasonable case to be made that students should not have been kept out of school once the COVID pandemic had stabilized, claims that masks didn’t prevent infection in children are factually wrong. For example, a study of 33,000 pupils in eight school districts in Massachusetts found an infection rate of 11.7% for the unmasked compared to 1.7% for masked children.
Also in Massachusetts, a study compared the numbers of COVID infections between school districts where compulsory masking requirements were lifted with those where they were maintained. Before the statewide masking policy was rescinded, the trends in the incidence of COVID in the Boston and Chelsea districts — which retained masking requirements —were similar to trends in school districts that later lifted masking requirements. However, “after the statewide masking policy was rescinded, the trends in the incidence of Covid-19 diverged, with a substantially higher incidence observed in school districts that lifted masking requirements than in school districts that sustained masking requirements.”
Another key finding that impacts students, who are packed together day after day: The use of masks doesn’t just protect the individual, it multiplies the protection of the entire community. Dr. Katelyn Jetelina and Yale University ER physician Dr. Kristen Panthagani point out:
Viral transmission in a population is exponential. Even if masks only reduce the risk of transmission for each individual by a small fraction, when a community masks, those small effects compound exponentially across a population, making a big dent in cases. Just like compounding interest — a small change in the percentage makes a big difference down the road.
The choice is yours
Ideological skeptics are not about to be convinced by the accumulating evidence. Their objections are to authorities they see as violating their autonomy by dictating what they must do in the interest of society. However, their disinformation about various aspects of the COVID pandemic is a disservice to the public.
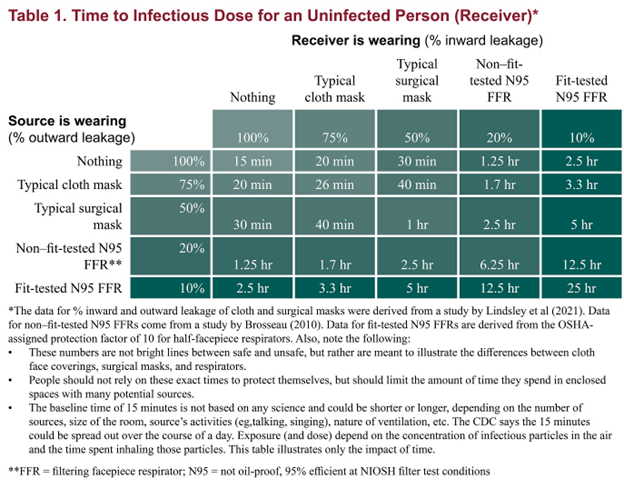
“It is completely understandable that the public and even the scientific community expresses confusion over how well masks protect against a respiratory disease like COVID-19,” noted a team of distinguished researchers at the University of Minnesota led by Michael Osterholm, the director of the Center for Infectious Disease Research and Policy (CIDRAP) and Regents Professor at the university. Their nuanced two-part discussion [here and here] is a valuable tool to challenge disinformers.
The team also produced the stunningly informative table below, which illustrates how long it would take for a person to be exposed to a virus when both a carrier and a non-infected person wear different types of masks versus when neither wear masks. Even a typical, cheap surgical mask worn by both parties offers four times the protection compared to neither person wearing a mask; that protection soars to a startling 100-fold greater — 15 minutes versus 24 hours — if both wear the highest-protection N95 mask.
Even if the latest increase in COVID cases, hospitalizations and deaths should prove transitory, we are not out of the woods. Another pandemic killer virus will come along, perhaps in our lifetime. If it does, we need to be prepared to utilize all reasonable measures to limit exposure. In July, Australian academic virologist Dr. Ian Mackay published a detailed, well-researched article on the effectiveness and importance of masks. It’s worth a read. He concluded:
[W]e each can take steps to reduce the amount of virus we get exposed to. Masks matter. A mask can help. So can clean or fresh air. As can distance. And these measures work against multiple very different airborne viruses and the diseases they cause. Reducing the infectious dose also means we may get a milder form of illness and still develop an immune response.
Dr. Mackay’s parting advice: “Wear a good mask well – reduce the [number of virus] particles you inhale. Masks matter.”
Acknowledgment: The author wishes to thank Jon Entine for his innumerable valuable suggestions and superb editorial assistance.
Note: A previous version of this artice was published by the Genetic Literacy Project.

Henry I. Miller, MS, MD
Henry I. Miller, MS, MD, is the Glenn Swogger Distinguished Fellow at the American Council on Science and Health. His research focuses on public policy toward science, technology, and medicine, encompassing a number of areas, including pharmaceutical development, genetic engineering, models for regulatory reform, precision medicine, and the emergence of new viral diseases. Dr. Miller served for fifteen years at the US Food and Drug Administration (FDA) in a number of posts, including as the founding director of the Office of Biotechnology.


