
Critical Economic Theory (CET) is taught at every business school in the country, but usually under the terms micro and macroeconomics. In any event, it is a lens to view issues. Like critical race theory, it has schools of thought biases, the broadest of which are capitalism vs. socialism. But today’s class is to share a few fundamental terms to consider the question:
Will lower drug prices hamper innovation?
Let’s begin with this graph from a recent article in Stat entitled, “Here’s who’s profiting the most in health care.”
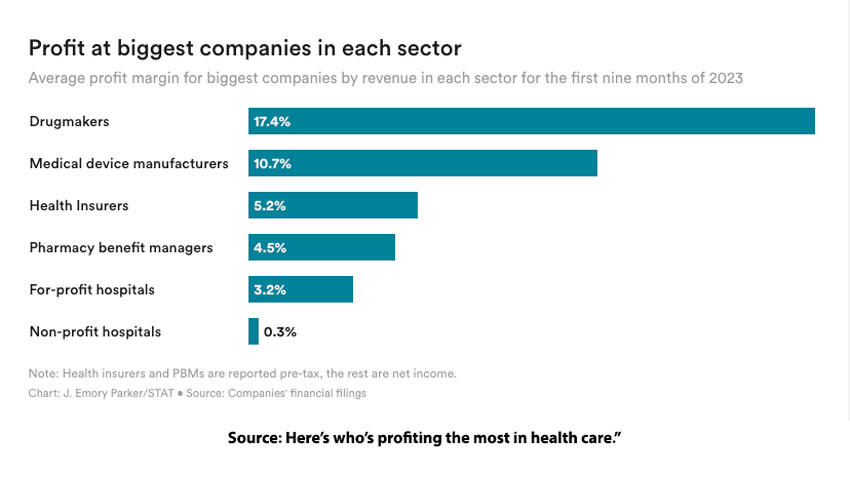
The average profit ratio or margin for pharmaceutical companies is 17.4%. What does that mean? There are at least three different ways to calculate profit ratios, but here we will deal with the one in the graph, net profit margin – the amount left after all the accounting is done. [1]
Revenue refers to the amount of money flowing into the corporation, primarily from the sale of its products, but revenue includes interest on investments. For comparison, your revenue is captured on those delightful W-2 forms and any interest you may have from investments like CDs and stocks.
Expenditures refer to the amount of money flowing out of the corporation, primarily the cost of goods (COGs), the materials used to manufacture medications, and operating costs. Operating costs include all the administrative costs, salaries, rentals, building maintenance, depreciation of equipment, payment of debt, and for pharmaceutical corporations, the cost of sales and marketing. More importantly, it includes the cost of innovation by their research teams and the companies they acquire.
For comparison, your expenditures include all the costs of living, housing, food, transportation, mortgage payments, and taxes. The one item not included in calculating your expenditures are those discretionary purchases, your wants, not needs. This is admittedly a fuzzy area; you may need to travel first class if for no other reason than it is more comfortable. Or you may need a more expensive car with room for six or seven, just in case. You can see how corporations might slide some luxury wants into their accounting of expenditures.
Net profits are the revenues remaining after all the expenditures. The net profit ratio expresses these profits as a percentage of sales. On average, large pharmaceutical companies retain a profit of $0.174 for every dollar of sales. It is more challenging to provide a comparison for an individual, but consider what you spend on the wants as your net profit.
Now, we can return to our original question. If the price of medications is lowered, will innovation suffer? Currently, for all the significant costs of drug development, including the drugs that fail to get out of the lab or past Phase I or II testing, and the crapshoot that is drug development, in short, the cost of innovation, pharmaceutical companies retain a significant profit.
According to Health and Human Services (HHS) spending on the ten most used medications by Medicare beneficiaries, those being considered for price reduction
“… more than doubled from 2018 to 2022 – a rate that was 3 times faster than all Part D drugs over the same period. The report also shows that 7 of the 10 drugs selected received direct at least one form of federal support towards their drug development or utilized a federal-funded invention for their development.”
There is no doubt that a price reduction will reduce pharmaceutical revenues, but the cost of current innovation is already baked in. A reduction in their revenue will reduce their profits, but not necessarily the operating costs of innovation. Big Pharma argues that they need prices to remain as elevated as they are, with America acting as the piggy bank for US-based global pharmaceuticals. Now, with the lens of Critical Economic Theory, you can have a more educated opinion or reframe the question. Should the price of drugs be adjusted for federal support towards drug development or the use of federally-funded inventions? Will investors be willing to take a bit less if it was to promote the common good?
Follow the Money – Health Insurance
The profit margin for health insurers is set at a maximum of 20% of sales – that is, 80% of all beneficiary revenue must be spent on beneficiaries’ healthcare costs. As the earlier graph shows, the net profit margin for health insurers is 5.4%, roughly 5 cents on the beneficiary payment dollar. Given what we just saw about net profit margins, you would think those insurance companies were lean, mean corporate machines. But CET teaches us that following the money is not always as easy as looking at revenue and expenditures.
United Healthcare and CVS Health (which owns Aetna health insurance and the largest pharmacy benefits manager[PBM]) are vertically integrated systems; they provide insurance, medications, and increasing health provider services. Money moves not so much in and out of United Healthcare or CVS Health but from the left to the right pocket. As Stat writes, “they routinely pay themselves for services, and the prices they set impact profitability.” In other words, some of United Healthcare’s profit comes from paying wholly owned PBMs large amounts that are recorded as expenditures by the PBMs but which ultimately contribute to United Healthcare’s unrecorded profit.
For Hospitals, Non-profit is not a Revenue Statement. It is a tax status
Non-profit hospitals, about 58% of all community hospitals, had the lowest profit margin, 0.3% - not even a penny on the dollar. Using our CET lens, we see why what constitutes revenue and expenditures varies in the non-profit world. These hospitals are exempt from “federal and state taxes, property taxes, sales tax, have special treatment for other taxes such as unemployment insurance, and may receive tax-deductible charitable contributions…”
The Kaiser Family Foundation estimates that the tax savings in 2020 were $28 billion, a little over half from relief from federal corporate taxes and the rest from state and local taxes. While it is easy to see why we would remove those savings from the expenditure column, hospitals argue that those savings should not become revenue. Why? In exchange for their tax exemption, non-profit hospitals provide “charity care,” steeply discounting or eliminating the cost of services for those unable to pay and other activities, initiatives, and investments to “improve the health of their communities.” [2]
Like our prior discussion of the fuzziness of the wants and needs of corporations, community benefit is often in the eye of the beholder. Charity care, writing off “costs” not covered by insurance or only partially covered, e.g., Medicaid was only $16 billion of that $28 billion, but they are the most straightforward benefit to identify. As a study reported by Stat states,
“38.5% of non-profit hospitals did not provide more community benefit, and 86% did not provide more charity care than the value of their tax exemption.”
To be fair, the American Hospital Association argues that it provides $9 in community benefits for every dollar of tax exemption. According to a study they commissioned
“Nearly half of those total community benefits, $51.1 billion, were comprised of financial assistance, unreimbursed Medicaid and other unreimbursed costs from means-tested government programs”
However, those write-offs reflect hospital sticker price, not the actual amounts paid by commercial or government insurance or the true costs of those services. Those write-downs are inflated, often 5-10 fold.
Understanding the economics of our form of capitalism, having the lens of CET or an introductory course in economics makes us better prepared to understand how our world works. Keeping us poorly equipped to follow the money makes us susceptible to both sides' sound bites and half-told tales. Sy Syms was right when he said, “An educated student is our best customer.” Economic education is vital for an informed electorate. [3]
[1] There are also gross profit margins and operating profit margins, which differ in which values are considered.
[2] This can include help with housing, access to nutritious foods, educational programs, health screenings, transportation of medical appointments, etc.
[3] There are many online free economics courses to consider. I like the work of Marginal Revolution University. Here is a sample

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


