
I have nothing against Vertex — quite the opposite. If you were asked to name five "really smart drug companies," it would be on many lists, including mine. Now, the company has a shot at getting FDA approval for a drug in the first novel class of pain medications in forever. Maybe. The question is: How well does VX-548 work; the answer is unclear.
In today's press release, the company announced Phase III results of VX-548, aka Suzetrigine, its novel non-opioid drug for treating moderate-to-severe pain following two especially painful surgeries (1). First, the good news.
“Treatment with VX-548 led to statistically significant improvement in pain compared to placebo as well as a clinically meaningful reduction in pain from baseline in both the abdominoplasty and bunionectomy randomized controlled trials.
- Treatment with VX-548 was also shown to be effective in the single-arm study in a broad range of surgical and non-surgical pain conditions for up to 14 days
- VX-548 was safe and well tolerated in all three studies
- Vertex plans to submit a New Drug Application to the FDA by mid-2024.”
Vertex press release, 1/31/24
Now, the bad news
As a key secondary endpoint, Vertex tested the hypothesis that VX-548 was superior to hydrocodone bitartrate/acetaminophen (Vicodin) on SPID48 (2) following abdominoplasty surgery or bunionectomy surgery. Neither trial met this critical secondary endpoint.
Here's a problem that was not explicitly mentioned. Not only did VX-548 fail to demonstrate superiority over Vicodin, but also that of the two most common oral opioids given following surgery, Percocet (oxycodone) and Vicodin – Vicodin is the weaker drug. Furthermore, the dose of Vicodin used in the trial was 5 mg – the lowest therapeutic dose of the drug. So it's safe to say that VX-548/Suzetrigine will not fare better against a more potent opioid and/or higher dose.
Does it work at all?
It would be hard to argue, especially based on the chosen time intervals that the drug has any effect in relief of pain following bunion surgery. The pain reduction scores track with placebo while the scores for Vicodin drop quickly, as would be expected. For some reason (possibly statistical – see below) VX-548 and Vicodin converge at 8-48 hours. I don't know exactly what to make of this, but waiting eight hours, let alone two days, for relief from a very painful surgery is very far from ideal (Figure 1).
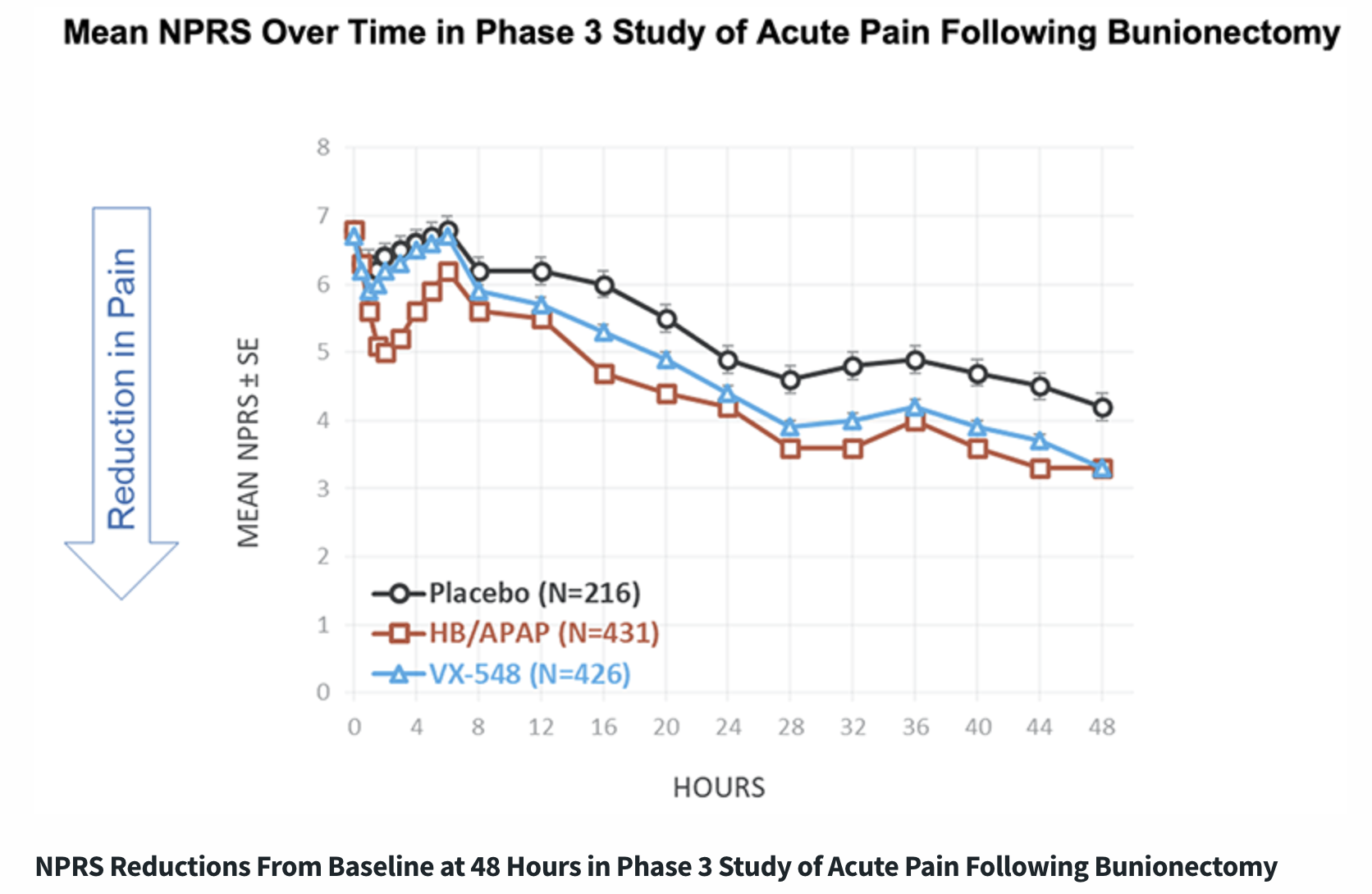
Figure 1. Efficacy against bunionectomy pain. Note that VX-548 appears to be indistinguishable from placebo until 8 hours following surgery.
Or are we just looking at "funny statistics?"
Dr. Jay K Joshi, practicing physician and contributor to Daily Remedy, has his own (rather cynical) take on Vertex's data:
Their pain evaluations were derived based on a time-weighted average. This is equal to the sum of the portion of each time period (as a decimal, such as 0.25 hour) multiplied by the levels of the substance or agent during the time period divided by the hours in the workday (usually 8 hours).
So acute exacerbations of pain, which are likely variable and obviously elevated in the short term, are heavily skewed toward pain scores in the early hours. But they chose to use an 8 hour and 48 hour time horizon at which point the latter pain scores, which would be obviously lower, have less of an impact in the total success metric.
All things considered, they used a measurement technique that heavily weighs short term pain, but then used time horizons for longer term pain evaluation. It would seem to me that they should either develop an observational study that has a shorter time horizon if they're going to use time-weighted averages, or use a traditional average pain score evaluation over a longer time horizon.
Why did the company overemphasize short term pain but use a long term time horizon? Spoiler: I know why. They wanted the perfect time horizon that would give them the statistical significance that they needed in order to make their results appear clinically meaningful.
Dr. Jay K. Joshi, private communication, 1/30/24
All is not lost
Although a non-opioid drug for post-operative pain would represent an important advance (3) it appears that VX-548 doesn't do the job. But all is not lost. There is an urgent need for an NSAID alternative in treating moderate, chronic pain caused by arthritis and a host of other conditions. Could VX-548 fill this void?
Vertex writes:
“Vertex conducted an additional Phase 3 study in 256 patients to evaluate safety and effectiveness in a broad range of surgical and non-surgical moderate-to-severe acute pain conditions. Treatment with VX-548 administered orally.”
Perhaps this is just as interesting...
Bottom line
It is doubtful that VX-548 will replace morphine or oral opioids following painful surgery (or perhaps any surgery). Still, the possibility of an NSAID replacement for chronic or acute aches and pains, headaches, etc., may be viable, although one cannot tell from the information that Vertex has released. This alone would represent a considerable advancement in the treatment of pain. But it's just too soon to tell.
Disclaimer: I neither own Vertex stock nor plan on having a bunionectomy or abdominoplasty in this or any other lifetime.
NOTES:
(1) Bunionectomy and abdominoplasty (tummy tuck) were not chosen at random. They are both notoriously painful operations.
(2) SPID48 is a method for measuring pain. Here is a simple definition: "The NPRS [Numerical Pain Rating Scale] can be used to assess the pain intensity difference (PID) and the summed pain intensity difference over 48 hours (SPID48), which are common primary efficacy endpoints in acute pain clinical trials."
(3) This is because some patients cannot tolerate opioid side effects, not because of addiction concerns, which is one bogus claims made by the usual idiots)

Josh Bloom
Director of Chemical and Pharmaceutical Science
Dr. Josh Bloom, the Director of Chemical and Pharmaceutical Science, comes from the world of drug discovery, where he did research for more than 20 years. He holds a Ph.D. in chemistry.


