
In the Annual Review of Medicine, Nalbandian and colleagues summarized Long COVID symptoms as shortness of breath, fatigue, brain fog, autonomic dysfunction, headache, smell or taste disturbance, myalgia, 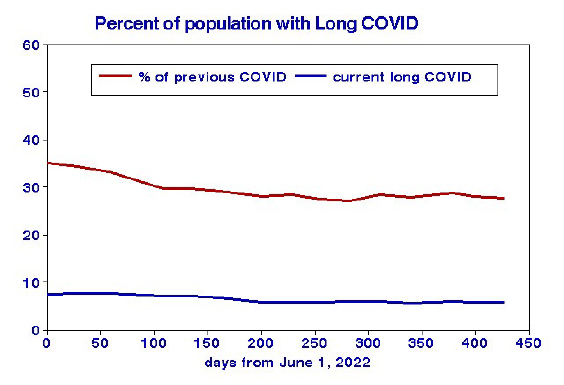 anxiety or depression, palpitations, and decreased functional capacity. It has been studied globally, and given the diversity of these locales and populations, it seems unlikely that any one set of socioeconomic predictors could be universally applicable.
anxiety or depression, palpitations, and decreased functional capacity. It has been studied globally, and given the diversity of these locales and populations, it seems unlikely that any one set of socioeconomic predictors could be universally applicable.
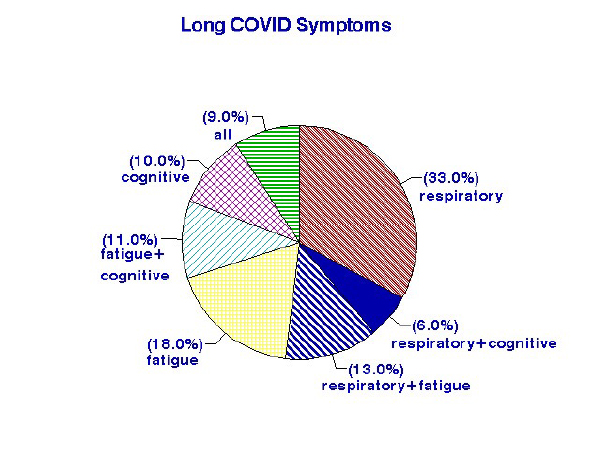
Previous studies of Long COVID have not identified durations of these highly variable symptoms, but the lower line for “current” Long COVID status indicates only modest duration. A cohort study reported symptom probabilities of 11% at 12 months after a positive test, decreasing to about 8% after 48 months. Gender, age, and comorbidity were found to be significant risk factors. Among symptoms, respiratory effects dominate.
 The Census Bureau’s Household Pulse Survey from June 2022 through July 2023 includes data on Long COVID rates according to personal characteristics. Some groups had a higher incidence of Long COVID.
The Census Bureau’s Household Pulse Survey from June 2022 through July 2023 includes data on Long COVID rates according to personal characteristics. Some groups had a higher incidence of Long COVID.
- Younger ages, < 65 years of age
- Females
- Latinos and those with multiple ethnicities
- Education, < high school diploma
- Disabled.
My analysis of the incidence of Long COVID is based on the contiguous 48 states and the District of Columbia, with the consistent denominator of those with a prior COVID infection (% had COVID). I first identified individual 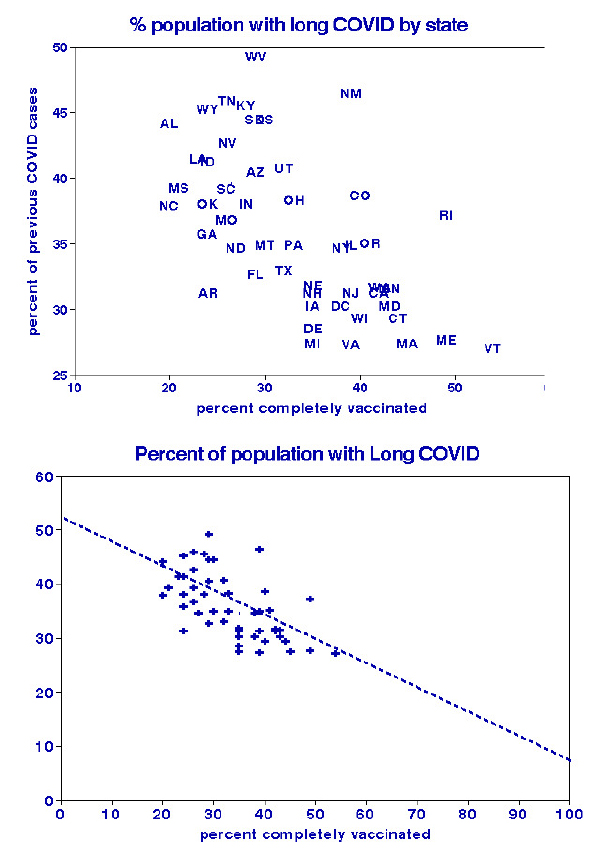 states’ cumulative Long COVID status and vaccination rates as of July 26, 2023. Northeast states were more highly vaccinated and had lower Long COVID rates than Southern or Western states. Benefits to the general public appear modest, but the benefit to those with previous COVID cases is striking and suggests that complete vaccination may have conferred immunity. However, high-vaccination states differ from low-vaccination states in many other ways.
states’ cumulative Long COVID status and vaccination rates as of July 26, 2023. Northeast states were more highly vaccinated and had lower Long COVID rates than Southern or Western states. Benefits to the general public appear modest, but the benefit to those with previous COVID cases is striking and suggests that complete vaccination may have conferred immunity. However, high-vaccination states differ from low-vaccination states in many other ways.
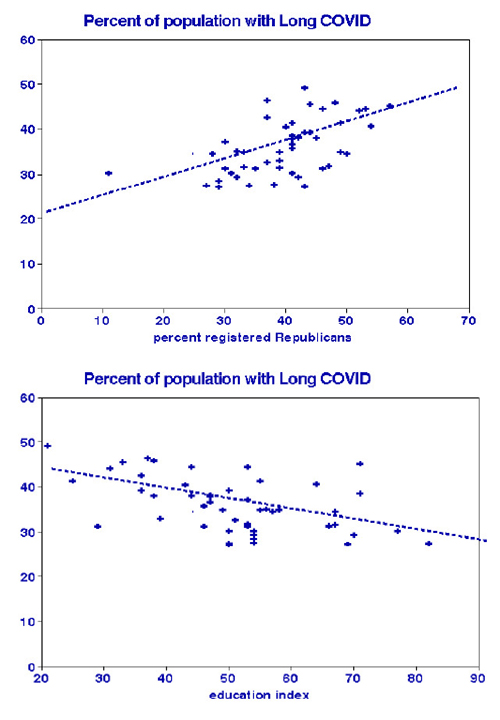 Other factors to consider include political affiliation and education. The graph indicates that registered Democrats may have Long COVID rates as low as 20% of previous cases, while rates for registered Republicans might be extrapolated to 70%. This may simply reflect vaccination; our previous analysis indicated that Republicans were vaccinated at much lower rates than Democrats.
Other factors to consider include political affiliation and education. The graph indicates that registered Democrats may have Long COVID rates as low as 20% of previous cases, while rates for registered Republicans might be extrapolated to 70%. This may simply reflect vaccination; our previous analysis indicated that Republicans were vaccinated at much lower rates than Democrats.
These graphs indicate that a variety of socioeconomic conditions may be predictive of Long COVID. I used statistical regression analysis to compare these and other population characteristics identifying the combination that best predicted Long COVID.
The best regression equation was a combination of vaccination status, political persuasion, and education, with an overall correlation coefficient of 0.70 and a prediction error of about 12%:
Percentage Long COVID = 38.5 +0.25 %Republican – 0.16 %vaccination – 0.14 education index
I evaluated potential predictors of Long COVID rates in terms of precision (percent error). Race, household crowding, and obesity were not statistically significant. Ambient air quality, comorbidities, population density, 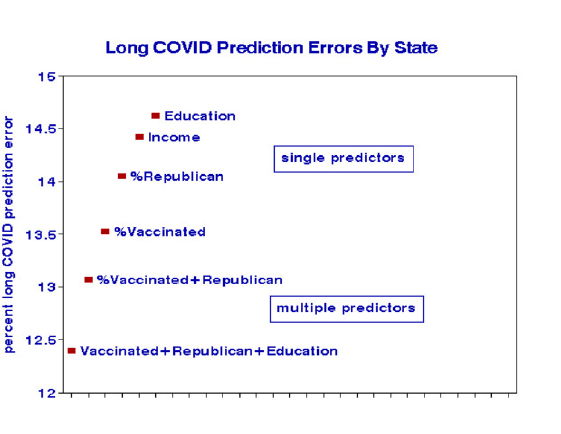 and gross domestic product (GDP) were of marginal significance. Significant variables with the least prediction errors shown in the chart were essentially behavioral and interrelated.
and gross domestic product (GDP) were of marginal significance. Significant variables with the least prediction errors shown in the chart were essentially behavioral and interrelated.
The least reliable of them is the education index, which was formulated arbitrarily. However, we may have underestimated the actual effects of education on incurring Long COVID.
Takeaways
It is not surprising that (lack of) vaccination was the best predictor of statewide Long COVID among previous victims of acute COVID or that politics and education participated in that relationship. Those variables are strongly intercorrelated, and the multiple regression results could be interpreted as indicating that Republicans and the less educated may suffer from increased vaccine hesitancy, so that vaccination is the main actor. These statewide relationships do not mean that changing political registration or returning to school would save one from Long COVID. The efficacy of vaccinations against acute COVID has been demonstrated in the laboratory and in clinical trials; our statewide epidemiology results extend those findings to reality in the field. Our dose-response graph shows that prior vaccination may reduce Long COVID by about 60%.


