
Concerns about breathing wildfire smoke continue and are often accompanied by dire predictions of imminent mortality based on statistical relationships. However, those estimates are incompatible with previous high-pollution episodes during which individual victims were identified and autopsied; it now seems appropriate to revisit those events. There is an ongoing epidemiology conundrum: large populations are required to achieve statistical significance (reduced noise). However, the larger the group, the less we can know about its individuals (increased bias and confounding). These previous episodes comprise one end of that distribution.
The Donora Polluted Fog Episode
Donora, Pennsylvania, was hit by a 4-day dense polluted fog in October 1948, trapping fumes from local industries. A previous article discussed subsequent peak illness and death rates that increased about 20-fold during the episode. The event achieved national prominence, with articles in the New York Times, the New Yorker, and the local press. There was also an extensive report from the US Public Health Service and several hard-cover books.[1]
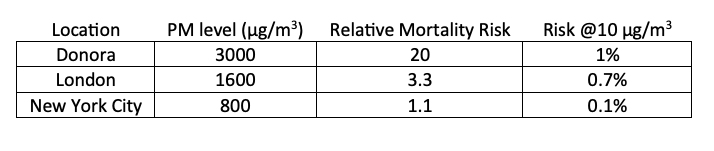
The fog penetrated indoors, sickening about 2400 people; 20 people died during the four days, whereas only about one death would have been expected in this population. Likely pollution sources included a zinc smelter and a nail factory. No environmental data were available, but airborne particulate levels were estimated at 3000 µg/m3, about 300 times the current US standard. A subsequent epidemiology report compared the fates of survivors and unexposed individuals.
Other Foggy Episodes
A dense fog occurred in December 1930 in the “half rural, half industrial” Meuse Valley near Liege, Belgium. Of the 9000 residents, 80 died on the 3rd and 4th days of fog, about 10-14 times normal. Local industries included coke, glass, steel, and sulfuric acid. Autopsies of 15 victims showed sooty lung deposits, and zinc oxide and fluorides were mentioned as possible toxic emissions.
During the notorious London fog of December 1952, smoke levels reached about 2500 µg/m3, and death rates approximately doubled. Domestic coal burning was identified as the primary emission source, and autopsies showed soot deposits in the lungs. New York City also suffered from high winter pollution during the 1950s and 60s, presumably from domestic space heating with heavy fuel oils. Local smoke levels may have reached 800 µg/m3 and penetrated residences and lungs. Excess mortality was estimated at 10%.
Summary of Major Episodes
To compare and provide perspective, I scaled these historical exposures to current ambient levels of 10 µg/m3 using straight-line relationships. Excess risks were less than 1% and similar to those reported from modern-day epidemiology studies over much longer periods.
Do These Events Leave Survivors At Increased Long-Term Mortality Risks (Residual Effects)?
The most detailed examination of this question was conducted in Donora. The Public Health Service reported autopsies showing acute inflammation deep into the lungs. They concluded that prior chronic cardiovascular disease was a “prominent feature” and concluded that
“the fog was not of itself of lethal intensity for previously normal people.”
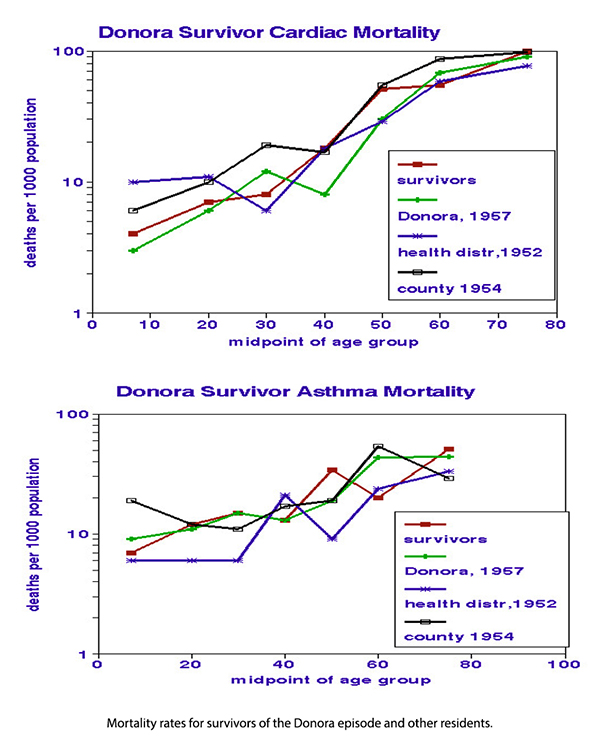 A study from the University of Pittsburgh compared subsequent mortality rates of survivors with and without fog symptoms, including residents of other areas. The graphics compare heart disease and asthma mortality rates by age groups for four independent sub-populations: Donora residents affected and unaffected by the fog, and individuals in the surrounding health district, and the county. Visual inspection indicates no consistent differences among the four groups; statistical analysis shows a slight cardiovascular advantage for the non-Donora residents. However, the most important finding is the absence of an ongoing “mortality penalty” as the fog survivors aged. This study concluded,
A study from the University of Pittsburgh compared subsequent mortality rates of survivors with and without fog symptoms, including residents of other areas. The graphics compare heart disease and asthma mortality rates by age groups for four independent sub-populations: Donora residents affected and unaffected by the fog, and individuals in the surrounding health district, and the county. Visual inspection indicates no consistent differences among the four groups; statistical analysis shows a slight cardiovascular advantage for the non-Donora residents. However, the most important finding is the absence of an ongoing “mortality penalty” as the fog survivors aged. This study concluded,
“No substantial or consistent relations between environmental and health experience could be demonstrated.”
Donora led to the recognition of a need for clean air. Various scientific conferences were held after Donora, but the first Federal clean air quality legislation was not enacted until 1963. It signaled growing awareness of environmental health and required the federal government to define air quality criteria to guide the curtailment of emissions based on scientific data. However, it was not until the 1970 Clean Air Act that the foundation for broadened federal authority, enforceable air quality standards, and routine ambient air quality monitoring began nationally. The episodes identified specific pollutants, metals, and black carbon that still have not been regulated while effectively ruling out contributions from ozone, nitrogen oxides, and hydrocarbons that are regulated.
Scant notice has been taken of these previous episodes; current air quality standards and regulations have been based on long-term geographic differences in ambient air quality and health statistics. Individual exposures and pre-existing medical conditions have not been considered, nor have delayed responses to cumulative exposures. Episode casualties comprised scientific evidence of lethality; purely statistical relationships do not.
[1] Shrenk H, et. al. Air Pollution in Donora, PA. Public Health Bulletin No. 306, Public Health Service. and Lipfert FW, Air Pollution and Community Health, Wiley, 1994


