
The folks at City Journal must not be aware of the Rule of Holes, “When you’re in a hole, stop digging.” Their contributors continue to make insupportable, easily disproved claims about the supposed lack of effectiveness of masks to prevent COVID-19.
Contributing editor John Tierney, unfazed by a thorough debunking of his first set of claims in February 2023 that masks don’t work to prevent COVID-19 infections, delivered yet another inaccurate, misleading rant six months later.
In the latter article, he presented – or I should say, misrepresented -- various studies and cherry-picked others. I responded in print to that article as well, discussing his errors at length.
Now, more than a year later, political scientist Jeffrey H. Anderson has popped up in City Journal with much of the same claptrap. He is exercised that
a handful of counties encircling the San Francisco Bay have announced new mask mandates in various health-care facilities for health-care workers in hospitals, skilled nursing facilities, or both, starting the day after Halloween and extending until early spring.
So, what is wrong with that? COVID infections are still occurring, and we’re bracing for a winter surge. (As of the CDC's last update on November 21, more than half of U.S. states reported moderate, high, or very high levels of SARS-CoV-2 virus, the etiologic agent of COVID-19, in wastewater.) For a start, Anderson believes that:
Americans shouldn’t be put in the position of potentially being tyrannized by one kingly official wielding largely unchecked powers. Yet the source of the mandates in at least three of these counties, and likely in all five, is a lone individual: the county health officer…
That, from a guy with no infectious disease, medical, or engineering training, mind you, but plenty of libertarian zeal. (As well as a tendency to exaggerate.)
Anderson goes on to provide “evidence” for his argument, which is of the “I did my research on the Internet, and now I’m an expert” genre:
Last year, [the Cochrane Library] found that wearing a mask ‘probably makes little or no difference to the outcome of laboratory-confirmed influenza . . . compared to not wearing’ a mask, and that using an N95 ‘compared to” a surgical mask ‘probably makes little or no difference for the . . . outcome of laboratory-confirmed influenza infection.’ Cochrane used the same language, verbatim, in its 2020 review.
Very well, let’s examine Cochrane’s meta-analysis of the effectiveness of masks. According to Anderson, it found that wearing masks does not prevent respiratory diseases, including COVID. I wonder whether he actually read the report, which was based on 78 selected studies, only six of which involved the COVID pandemic and only two of those specifically studied COVID and mask mandates. (Moreover, those two were concerned only with whether mask mandates were in place but not actually with the wearing of the masks.)
But here’s the most important part… The Cochrane report itself identified these two statements as the “key messages” of their analysis: “We are uncertain whether wearing masks or N95/P2 respirators helps to slow the spread of respiratory viruses based on the studies we assessed,” and “[h]and hygiene programs may help to slow the spread of respiratory viruses.” (Emphasis added.)
Expanding on those summary statements, here are the first four sentences of the Cochrane authors’ conclusions:
The high risk of bias in the trials, variation in outcome measurement, and relatively low adherence with the interventions during the studies hampers drawing firm conclusions. There were additional RCTs [randomized, controlled trials] during the pandemic related to physical interventions but a relative paucity given the importance of the question of masking and its relative effectiveness and the concomitant measures of mask adherence which would be highly relevant to the measurement of effectiveness, especially in the elderly and in young children.
There is uncertainty about the effects of face masks. The low to moderate certainty of evidence means our confidence in the effect estimate is limited, and that the true effect may be different from the observed estimate of the effect.
Moreover, in the authors’ discussion of their findings about the effectiveness of the highest quality, most effective masks – N95/P2 respirators – there is no mention at all of COVID specifically.
Following the distortions and contortions of Tierney and others, officials at Cochrane clarified the results of their analysis -- specifically, admitting that the way it summarized the review was unclear and imprecise, and that the way some people interpreted it was wrong. This is from a March 2023 column in the New York Times, headlined "Here’s Why the Science Is Clear That Masks Work":
'Many commentators have claimed that a recently updated Cochrane review shows that ‘masks don’t work,’ which is an inaccurate and misleading interpretation,' Karla Soares-Weiser, the editor in chief of the Cochrane Library, said in a statement.
‘The review examined whether interventions to promote mask wearing help to slow the spread of respiratory viruses,’ Soares-Weiser said, adding, ‘Given the limitations in the primary evidence, the review is not able to address the question of whether mask wearing itself reduces people’s risk of contracting or spreading respiratory viruses.’
She said that ‘this wording was open to misinterpretation, for which we apologize,’ and that Cochrane would revise the summary.
Soares-Weiser also said, though, that one of the lead authors of the review even more seriously misinterpreted its finding on masks by saying in an interview that it proved ‘there is just no evidence that they make any difference.’ In fact, Soares-Weiser said, ‘that statement is not an accurate representation of what the review found.’
Other evidence of the effectiveness of masks comes from an extensive analysis published in The Lancet by several dozen researchers from six universities, which found:
State governments' uses of protective mandates were associated with lower infection rates, as were mask use, lower mobility, and higher vaccination rate, while vaccination rates were associated with lower death rates.
The benefit of masks was confirmed again by a study published last year by a distinguished group of British and Canadian scientists who performed a 'rapid systematic review of evidence [that asked] whether (i) wearing a face mask, (ii) one type of mask over another and (iii) mandatory mask policies can reduce the transmission of SARS-CoV-2 infection, either in community-based or healthcare settings. A search of studies published 1 January 2020–27 January 2023 yielded 5185 unique records.'
Their conclusion:
Despite the [risk of bias], and allowing for uncertain and variable efficacy, we conclude that wearing masks, wearing higher quality masks (respirators), and mask mandates generally reduced SARS-CoV-2 transmission in these study populations.
At the risk of stating the obvious, lower infection rates mean fewer illnesses, hospitalizations, deaths, and cases of long COVID – all important outcomes.
Michael Osterholm, the director of the Center for Infectious Disease Research and Policy (CIDRAP) and Regents Professor at the University of Minnesota, and his colleagues have provided a scholarly, two-part discussion of the nuances of wearing masks to prevent respiratory infections here and here.
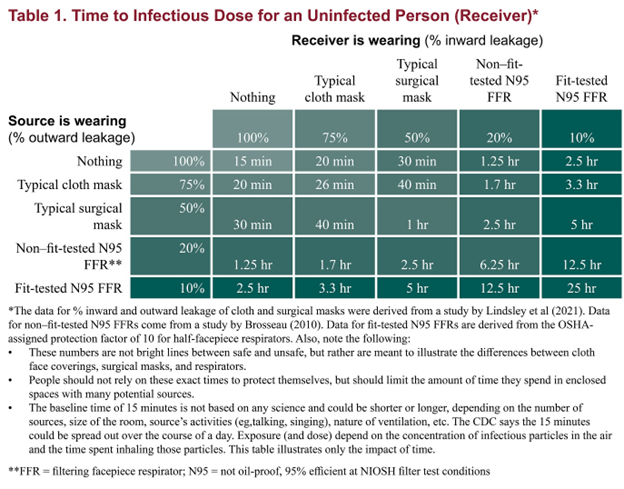
Additional persuasive evidence is found in the table below which illustrates the degree of protection against an aerosol afforded by different types of masks when worn by both source and receiver. It demonstrates that “an N95 FFR [filtering faceplate respirator, such as an N95], even if not fit-tested, offers more benefits as both source control and personal protection than any mask,” as measured by the time it takes until] an infectious dose is received:
There’s much more.
As Drs. Katelyn Jetelina and Kristen Panthagani included this important point in an excellent article on the ability of masks to prevent the transmission of viral respiratory diseases:
Viral transmission in a population is exponential. Even if masks only reduce the risk of transmission for each individual by a small fraction, when a community masks, those small effects compound exponentially across a population, making a big dent in cases. Just like compounding interest — a small change in the percentage makes a big difference down the road.
Finally, they discuss the palpable weaknesses of the Cochrane meta-analysis so beloved by Tierney and Anderson, including:
- The trials in the Cochrane analysis “had a number of problems and, given the limited number of RCTs [randomized controlled trials] on COVID-19, do not represent the totality of evidence.”
- The Cochrane analysis encompassed trials with different viruses: “When a virus is less contagious, an effect is harder to detect. Many of the RCTs evaluated influenza, which is far less contagious than COVID-19. This means that if we combine them, the impact of masks may be underestimated. (Another scientist, separate from this review, removed the flu studies and reran the meta-analysis. He found masks protected against SARS-CoV-2.)
- The Cochrane analysis combined studies performed in widely disparate settings. “Studies ranged from suburban schools to hospital wards in high‐income countries, crowded inner city settings in low‐income countries, and an immigrant neighborhood in a high‐income country.”
There’s more that Jetelina and Panthagani could have added, including the CDC’s compilation of studies of mask efficacy, which shows that most have found positive effects from masking. For example, a study of 33,000 pupils in eight school districts in Massachusetts found an infection rate of 11.7% for unmasked compared to 1.7% for masked children.
Also in Massachusetts, a study compared the numbers of COVID infections between school districts where compulsory masking requirements were lifted with those where they were maintained. Before the statewide masking policy was rescinded, the trends in the incidence of COVID in the Boston and Chelsea districts -- which retained masking requirements -- were similar to the trends in school districts that later lifted masking requirements. However, the researchers found that "after the statewide masking policy was rescinded, the trends in the incidence of Covid-19 diverged, with a substantially higher incidence observed in school districts that lifted masking requirements than in school districts that sustained masking requirements."
Virginia Tech engineering professor Linsey Marr explained in simple terms last year on CBS’s 60 Minutes how masks trap virus particles.
Finally, in 2022, Australian academic virologist Dr. Ian Mackay published a lengthy, well-researched article on the effectiveness and importance of masks. He concluded:
[W]e each can take steps to reduce the amount of virus we get exposed to. Masks matter. A mask can help. So can clean or fresh air. As can distance. And these measures work against multiple very different airborne viruses and the diseases they cause. Reducing the infectious dose also means we may get a milder form of illness and still develop an immune response.
Dr. Mackay’s parting advice: “Wear a good mask well – reduce the [number of virus] particles you inhale. Masks matter.” I agree with him.
Believe the scientists, not the cranks, ideologues, and armchair experts.

Henry I. Miller, MS, MD
Henry I. Miller, MS, MD, is the Glenn Swogger Distinguished Fellow at the American Council on Science and Health. His research focuses on public policy toward science, technology, and medicine, encompassing a number of areas, including pharmaceutical development, genetic engineering, models for regulatory reform, precision medicine, and the emergence of new viral diseases. Dr. Miller served for fifteen years at the US Food and Drug Administration (FDA) in a number of posts, including as the founding director of the Office of Biotechnology.


