
When demand exceeds supply, a resource is limited. Allocating those resources “involves a tension between efficiency and equity.” The market has several ways to allot those limited resources, beginning with cost, for example, frequent flyer miles, a form of resource allocation, may not seem controversial, except to those getting on last where there is no room for their carry-on. Health care is a limited resource for many reasons, and equity raises more significant ethical concerns.
Resource allocation involves hurdles to overcome, often termed frictions or pain points. Healthcare’s traditional frictions involved cost, time, and the moat created by office staff between you and your physician. While government insurance plans, Medicare and Medicaid, have leveled costs somewhat, time spent getting an appointment and then being seen, as well as the staff moat and automated telephone chains, remain significant frictions.
Concierge medicine is a new, small, roughly 7% practice style in the US, growing at 3 to 4% annually. Here’s the deal: in exchange for a retainer fee, most of the frictions concerning time and access are removed. You get the undivided attention of your primary care physician whenever you want – no waiting for appointments, no telephone waiting, no nurse practitioner physician assistant intermediaries.
Given the increased demands on healthcare as the Boomers age out, and the increasing physician shortage in different specialties and geographic locations, it helps to understand the impacts of concierge medicine.
Welcome to the Club
Concierge care requires a membership fee the patient pays as an out-of-pocket expense. The physician continues to bill the patient’s insurance for care but “waives” the out-of-pocket and deductibles that the patient is responsible for paying. With membership or retainer fees in the $2,000 annually range, physicians can significantly reduce the size of their practice “from roughly 2,500 to less than 600.” With fewer patients, care is, in economic terms, non-rivalrous; you can be seen at your convenience. A physician has created a substantial baseline income with an upfront cash membership fee.
“This new model may improve health outcomes if willingness to pay reflects the sensitivity of the patient’s health to improved access, and scarce provider time can be allocated to patients for whom increased attention is most beneficial.”
The ability to pay and the “need” for care influence how patients select in or out of concierge care. Income may serve as a proxy for the ability to pay, and need, at least for health issues, can be measured by visits and co-morbidities. To see the impacts, a new study in the Journal of Health Economics examines concierge care’s costs, participants, and health outcomes.
The Data Set
The researchers looked at over 800 physicians transitioning from traditional practices to concierge medicine, all affiliated with a single large company managing these transitions. Physicians retain ownership of their practice and generate revenue from insurer billing [1] and a retainer fee, on average $2400, with the company charging a percentage for administrative services. Patient “panels” are limited to 600, and the study was limited to Medicare beneficiaries, who had the most readily available health data. 28,000 Medicare beneficiaries were joining the concierge practice, “stayers,” and 123,000 were “leavers.”
“Collectively, these trends point to an increased amount of time spent with patients, on average, as would be expected under CM [concierge medicine].”
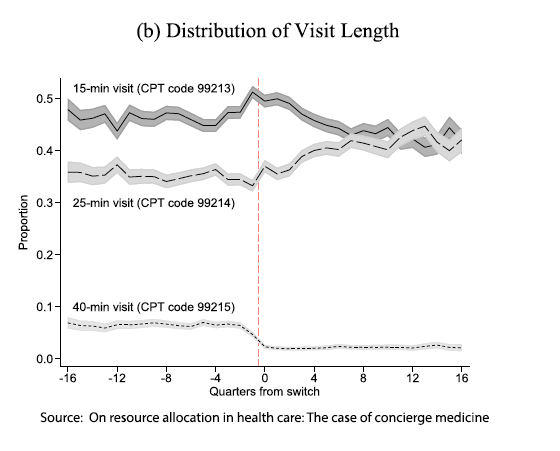
The graph shows how the proportion of visit length changed from before to after the transition to concierge care. 15-minute visits declined, and 25-minute visits increased. Interestingly, 40-minute visits also declined. However, this may reflect the impact of more frequent, shorter visits for “follow-up” and concerns.
“We find an increase in the out-of-pocket retainer fee reduces the proportion of members who derive health benefits from concierge medicine, as members sufficiently wealthy to enroll in concierge medicine join for reasons beyond health. Moreover, as the retainer fee increases, more individuals who are in poor health select out due to affordability.”
There was double the number of leavers as stayers. Both stayers and leavers experience increased spending, with the magnitude greater for the stayers even without including the concierge fee, a large component of the additional cost. Prescription drug costs declined for stayers, as more consistent care resulted in deprescribing, while outpatient and inpatient care costs rose. As the researchers write, “the magnitudes of the differences are not economically large.”
The stayers “are slightly older, have slightly fewer chronic conditions diagnosed…” They have more income as measured by living in higher-income zip codes and being unlikely to receive a low-income subsidy for drug costs.
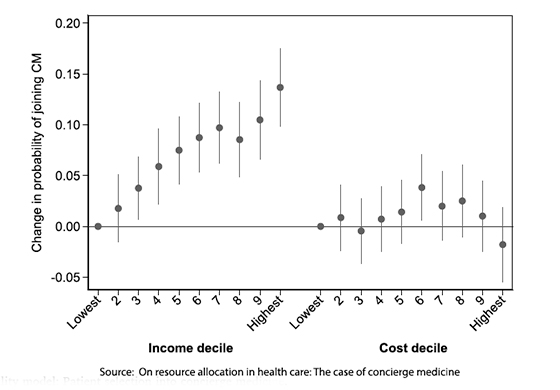 The graph on the left depicts the probability of a patient joining concierge care based on income and expected healthcare costs. As income rises, as measured by higher-income zip codes, the likelihood of participating in concierge care rises from a baseline of 28% in the lowest-income decile to a nearly 50% likelihood in the highest-income decile. Costs do not show a similar steady rise. When adjusted for income, only those in the 6th decile of expected cost were more likely to seek concierge care. The patients with the greatest expected costs were disinclined to seek concierge care.
The graph on the left depicts the probability of a patient joining concierge care based on income and expected healthcare costs. As income rises, as measured by higher-income zip codes, the likelihood of participating in concierge care rises from a baseline of 28% in the lowest-income decile to a nearly 50% likelihood in the highest-income decile. Costs do not show a similar steady rise. When adjusted for income, only those in the 6th decile of expected cost were more likely to seek concierge care. The patients with the greatest expected costs were disinclined to seek concierge care.
Let me add a limitation to those findings that the researchers did not mention. The largest of the concierge management groups assisting a practice in transitioning to concierge care carefully reviews and determines the “best” candidates to invite into the concierge care patient panel. They optimize for patients with the best possible insurance and the fewest medical problems, what we might call the “concerned well.” A physician may include some additional patients of their choosing in the invitation to the concierge practice. The findings regarding who opts into concierge care may reflect a selection bias attributable to concierge management rather than a patient’s “free will.”
“On average, there is no meaningful difference in survival for patients whose physician switches to CM [concierge medicine].”
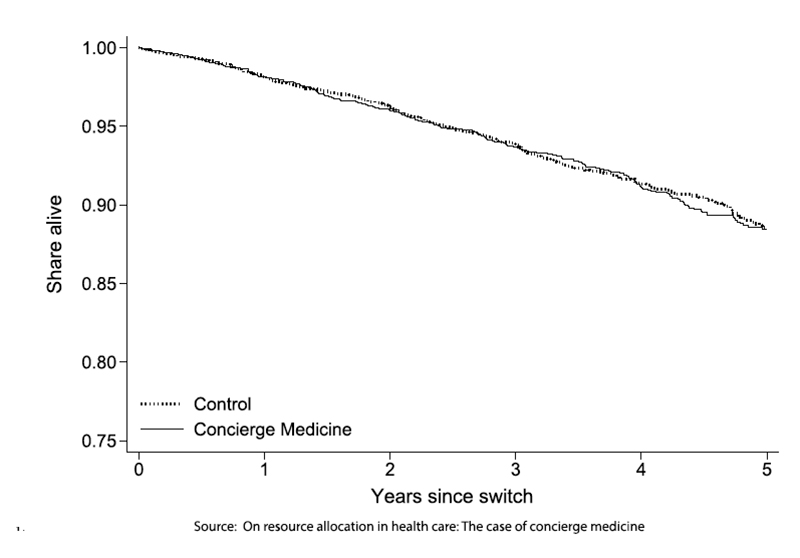
The graph shows the five-year survival of those patients with concierge care, the stayers, vs. those of the same physician who did not participate in concierge care, the leavers. Over the five-year interval, concierge medicine increased survival by “less than 2 days.” A deeper dive suggested that the risk to survival for those patients with the greatest co-morbidities was worse with concierge care, but the numbers were too small to identify any statistical, let alone clinical, validity. It is reasonable to argue that the five-year window, one-quarter of the life expectancy of a 65-year-old Medicare recipient, is insufficient to see a clinical difference
“Our paper has three main findings. First, there is limited patient selection into concierge medicine based on health status. We find evidence that income (at the level of patient zip code) has a stronger influence on the decision for patients to pay the retainer fee to join. Second, concierge medicine increases total healthcare spending. The increase is large starting in the year after the switch and grows to 30–50% higher compared to before the switch. Third, we find no evidence that concierge medicine leads to mortality changes, on average.”
For physicians, the goals of concierge medicine are clear and easily achieved. The concierge fee places a guaranteed lower bound on their income; they will see fewer patients more engagingly and may find a better “work-life” balance. To the extent that it can extend the professional career of older physicians who might have otherwise dropped out of the workforce or increase income in primary care to the point that it is competitive with specialty care, it can improve access to care. [2]
The findings for patients are more ambiguous. Patients receive more time and attention, and while it is not measured in the study, the frictions of waiting and appropriate referral are reduced. However, concierge medicine does not appear to reduce these frictions for “people in worse health and those living in lower-income areas,” exacerbating disparities already present. Additionally, with fewer patients per physician, concierge care shifts more patients into already stressed practices.
Concierge medicine offers a tantalizing promise of premium healthcare service. For those who can afford it, the benefits of immediate access and personalized care are apparent. However, the model raises significant concerns about equity in providing care to those most in medical need. The real question is whether this exclusive club can coexist with a system that should strive for both efficiency and fairness.
[1] Physicians offered extended office visits, same-day appointments, increased phone/email access, comprehensive health screenings, diagnostic tests, and “online access to their personal health records, including summaries of their visits, lab results, EKGs, and other medical information.”
[2] In one study seeking to understand the impact of the retirement of a primary care physician on their patients, researchers found that adverse consequences increased, including a roughly 4% increase in ED visits, hospitalizations, and deaths. As they write and I have argued, the patient-physician relationships “contain non-transferable information that positively impacts patients’ health.”
Source: On resource allocation in health care: The case of concierge medicine Journal of Health Economics DOI: 10.1016/j.jhealeco.2023.102776

Chuck Dinerstein, MD, MBA
Director of Medicine
Dr. Charles Dinerstein, M.D., MBA, FACS is Director of Medicine at the American Council on Science and Health. He has over 25 years of experience as a vascular surgeon.


